
This post tackles two RxISK themes – ADHD and Polypharmacy.
While working through Pfizer’s Serious Adverse Event narrative file, see The Fog of a Special Medical Operation, the term ADHD – attention deficit hyperactive cropped up quite often.
There was one predictable feature to this – all cases came from the United States with none at the moment from Argentina, Brazil, Germany, Turkey or South Africa. The numbers are relatively small but there appear to be more Serious Adverse Events in the vaccinated group than in the placbo group in those on treatment for ADHD. Beyond the serious Adverse Events File, there are roughly equivalent numbers – but we need more work on this.
What we don’t know from this is whether there is a particular ADHD treatment linked to serious events. We searched on ADHD – not even attention deficit or any related terms. We did not search on stimulants – which might yield more cases. All the cases below apparently have ADHD.
Note the ages of those involved.
Serious Adverse Event Group
- Unique Subject ID: C4591001 1134 11341153; USA: BNT162b2 (30 μg) 44 F safety withdrawal
- Unique Subject ID: C4591001 1006 10061098; USA: BNT162b2 (30 μg) 66 F SAE
- Unique Subject ID: C4591001 1097 10971061; USA: BNT162b2 (30 μg) 67 F SAE
- Unique Subject ID: C4591001 1167 11671175; USA: BNT162b2 (30 μg) 55 M SAE
- Unique Subject ID: C4591001 1178 11781015; USA: BNT162b2 (30 μg) 67 M SAE
- Unique Subject ID: C4591001 1178 11781048; USA: Placebo 59 F SAE
- Unique Subject ID: C4591001 1081 10811194; USA: Placebo 51 F Death
Other Trial Volunteers
- Unique Subject ID: C4591001 1046 10461058; USA: Placebo 44 F Covid
- Unique Subject ID: C4591001 1068 10681082; USA: Placebo 58 M Covid
- Unique Subject ID: C4591001 1079 10791054; : USA: Placebo 28 F Covid
- Unique Subject ID: C4591001 1088 10881233; USA: Placebo 47 M Covid
- Unique Subject ID: C4591001 1123 11231085; USA: Placebo 20 M Covid
- Unique Subject ID: C4591001 1125 11251238; USA: Placebo 17 F Covid
- Unique Subject ID: C4591001 1169 11691058; USA:Placebo 32 M Covid
- Unique Subject ID: C4591001 1110 11101050; USA: BNT162b2 (30 μg) 47 M Covid
- Unique Subject ID: C4591001 1091 10911387; USA: BNT162b2 (30 μg) 17 F Covid
We know there are other cases. Maddie de Garay and her siblings, all of whom were in the Pfizer children’s trial have ADHD and were on treatment but do not feature here. The trial we are looking at here is adults only.
Patrick Hahn (author of Obedience Pills) Your Country Needs You to review these cases and tell us more and perhaps find out if there are more cases by searching under individual drug names using Abstractor
Polypharmacy
What was also clear was that some of those entering this trial were on a great deal of other medication.
- levetiracetam (since 2003) for seizure disorder.
- quetiapine (since 2010) for bipolar disorder,
- paroxetine (since 2010) for anxiety,
- butalbital/caffeine/
paracetamol (since 2010) for migraines - topiramate (since 2013) for migraines,
- gabapentin (since 2013) for low back pain
- oxycodone/paracetamol (since 2016) for low back pain,
- buspirone (since 2014) for depression,
- baclofen (since 2018) for muscle spasms,
- ropinirole (since 2018) for restless leg syndrome,
- fish oil and vitamin D2 (since 2019) as vitamin supplements,
- atorvastatin (since 2019) for hyperlipidemia,
- cetirizine (since 2019) for seasonal allergies,
- albuterol inhaler (since 2020) for shortness of breath.
- blood potassium decreased,
- Escherichia coli urinary tract infection,
- nephrolithiasis
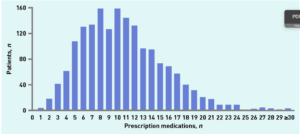
The Serious Adverse Events Narrative (Sensitive) file contains roughly 288 placebo cases and 190 vaccinated cases. Pfizer were good at recording other meds people were on and conditions they had – it helps introduce Fog into the Field of Battle ( see The Fog of a Special Medical Operation).
Each patient has roughly 10 pages to their name with the drugs in the narrative on the next to last page – the page that tells you how Pfizer made these patients disappear.
It would be fascinating to get an average number of drugs per person in this Adverse Event file. Working on this isn’t hard – it can be a great way to while away a few hours.
Get in touch if you can help. We don’t want too much duplication – so this will need some co-ordination, unless someone finds it soothing – like knitting – and you find you can’t stop.
People Acknowledgement
RxISK acknowledges that the experiences of those who have been harmed by medical treatments are the cornerstone on which it is built, and believes this should be the case for all of medicine.
See Black Robe, White Coat for more detail on this people acknowledgement
Pogo says
Fog indeed. Analogous to what we in Britain call a green pea-souper, compleate with a sulphurous smell and taste.
I would be inclined to suspect that cases have only shown up so far in the US because:
1. Peolpe even with mild cases of ADHD are more likely to get diagnosed in the US.
2. More likely to be offered treatment in the US.
3. The highest immunisation schedual in the world is in the US.
Therefore, a significant majority of those with ADHD may have it as a result of previous inoculations progressively damaging their immune system. This would leave such people (one would think) more likely to suffer severe advers reaction on receiving yet another assault (shot) to their immune system.
Someone, a few years back collected and collated data from diffrent counties showing the increase in ADHD, autoimmune disorders, late onset autism, etc. which rose in proportion with each countries vaccine schedule.
Whilst authorites put this down to changing enviromental factors, the very medical intervention designed to have an effect the immune system are vigorously ignored. Any evidence shown to them that should raise red flags are dismissed with “ correlation is not proof of causation”.
I’ve forgotten where I came across this data and graphs showing these increases but have found this….
On slide 8 it compares the infant mortality rate against the vaccine schedule for 34 counties. On slide 46 it gives the cumlative number of office visits to a healthcare provider for ADHD between vaccinated vis. unvaccinated. Must point out though that this graph (and for the Hooker-Miller study mentioned on other slides) is based on a very small cohort (although magnitudes greater than six mice, which was thought sufficient to approve the latest Cover shot), so the results are open to question by the authorities regarding demographic biases, etc.
https://totalityofevidence.com/wp-content/uploads/2022/07/Dr-Paul-Thomas-presentation-slides-Health-Freedom-Summit.pdf
Still. This is not to say I think the biologicals (the shots) must take all the blame and the pharmalogicals can be ignored, as I don’t think there is any argument about stimulants ability to have a deleterious effect on the immune system and some may be worse than others.
annie says
REVEALED: The hidden epidemic of sexual dysfunction which experts blame on SSRI antidepressants
SSRI antidepressants could cause ‘life-changing’ sexual problems experts say
1 in 8 people were prescribed antidepressants in the past year according to stats
But they can cause serious side effects like libido drop and numb groin areas
Many report they no longer experience sexual or romantic attraction at all
By JO MACFARLANE FOR THE MAIL ON SUNDAY
PUBLISHED: 22:00, 1 October 2022 | UPDATED: 22:00, 1 October 2022
https://www.dailymail.co.uk/health/article-11269871/The-hidden-epidemic-sexual-dysfunction-experts-blame-SSRI-antidepressants.html
Patients on antidepressants are not being warned of the risk that the pills could permanently ruin their sex lives, experts say.
The Mail on Sunday has been contacted by a number of patients who claim to have been left with ‘life-changing’ sexual problems after taking a class of the drugs known as selective serotonin reuptake inhibitors (SSRIs) to ease symptoms of depression and anxiety.
In the past year, about one in eight people in the UK were prescribed antidepressants, which includes SSRIs, according to the latest official figures – a number that has soared since the pandemic.
They can prove transformative for many people, but are linked with side effects. It has long been known, for example, that those taking them, both men and women, can experience a drop in libido.
But some patients claim the effects have been more persistent and have continued, or even worsened, years after they stopped taking the drugs. Some have had problems for decades.
The symptoms they describe are strikingly similar. Genital numbness – a total lack of sensation around the groin – and for men, erectile dysfunction. Both men and women experience a condition known as anorgasmia – a difficulty in reaching orgasm, and if they do climax, it is weak or without pleasure. As one woman put it: ‘It’s like a sneeze.’
Many report they no longer experience sexual or romantic attraction at all, and have been left with an emotional numbness. Most have seen relationships collapse as a result, while others have missed out on the chance to have children. Some have never experienced pleasure during sex – called anhedonia – and worry they never will.
CRY FOR HELP: Powerful images from the PSSD Network’s campaign
Significantly, all have found their symptoms repeatedly dismissed by medical professionals, who insist they are linked to their underlying depression and not the pills.
One 22-year-old, a student in London, described how his problems began after he stopped taking a low dose of SSRI drug escitalopram for exam stress last year.
Speaking to The Mail on Sunday on condition of anonymity, he said: ‘My penis is basically inanimate. Any attraction I might have felt to any woman has disappeared. If I try to have sex, I might as well be doing the dishes.
‘This area of my life used to be so much fun, and now it’s a source of anxiety and has become a dark place in my head. It feels like someone has gone into my brain with a scalpel, carved some bits out and left me with this strange, numb, asexual person.
‘No doctor will even consider that it might be related to the SSRI.’
Rebecca Graham is in her early 40s and has had no sensation in her genitals for eight years since she came off the SSRI drug sertraline, which she had been prescribed for symptoms of premenstrual syndrome. She has sought help from ‘around ten specialists’, from counsellors to gynaecologists, without success. ‘My whole genital area is numb,’ she says. ‘I feel like I’ve been castrated.
‘I thought things would improve, but they never did. My partner and I live as best friends and I’ve given up on the idea of children. I’ve been told SSRIs don’t cause numbness, that no condition could explain my symptoms but that a lot of emotions control that area of the body. It’s like being gaslit by the medical profession.’
And this is the heart of the issue. While what these patients have experienced is recognised in the medical literature – and even has a name: post-SSRI sexual dysfunction, or PSSD – there is little evidence or research that proves a definitive link to the drugs.
David Baldwin, professor of psychiatry at the University of Southampton, cautioned that doctors still don’t know whether PSSD is caused by SSRIs or is a symptom of recurring depression or anxiety.
However, he added: ‘If a patient has sexual dysfunction long after stopping SSRI treatment, and this occurs in the absence of depressive or anxiety symptoms, it could be they are experiencing PSSD.’
Data released last week under Freedom of Information laws by the Medicines and Healthcare Products Regulatory Agency watchdog shows that one in five of 1,762 reports of sexual dysfunction associated with SSRI use continued after stopping the drugs. In fact, in 64 per cent of reports, the MHRA confirmed that it remained ‘unknown’ whether the problem had persisted.
An increasing number of experts say there is enough evidence to show post-SSRI sexual dysfunction is plausible but that further work is needed to evaluate the risks.
Dr Joanna Moncrieff, professor of critical and social psychiatry at University College London, says: ‘The majority of people taking SSRIs will get some form of sexual dysfunction – there’s no debate about that.
‘They’re prescribed to sex offenders to curb their libido, so it isn’t a huge stretch to imagine that symptoms persist.’
She adds: ‘The other thing that makes it convincing is all the evidence about prolonged withdrawal symptoms from SSRIs. If you take drugs for a long time, they alter the brain in ways that may be permanent, or at least takes a long time to normalise.’
In 2019, the EU’s drug watchdog, the European Medicines Agency, acknowledged the growing number of reports of post-SSRI sexual dysfunction, and added a new warning to leaflets inside the packaging.
But Dr Moncrieff believes these warnings are not filtering through to doctors and so are not being made clear to patients. ‘People need to be aware that we don’t know much about it – we don’t know how common it is and we don’t know how to treat it.’
A rise in the number of young people being prescribed antidepressants made these warnings ‘even more important’, Dr Moncrieff adds.
A new global pressure group, PSSD Network, launched an awareness campaign last week featuring powerful images of those suffering from the condition holding placards that describe the impact it has had on them.
One man who has taken part is Lee Edward. His placard, which partially obscures his face, reads: ‘Antidepressants saved my life… then ruined it.’
The 43-year-old, from Cannock, Staffordshire, started taking sertraline in 2017 after his father died. He experienced minor sex-related problems during the 18 months he was on the drug, but six months after he stopped taking it, in September 2019, the problem significantly worsened.
‘My penis was numb, and there was no pleasure whatsoever. Trying to have sex without those feelings of arousal was just weird. It was so awkward, just two bodies moving around.’
Blood tests and scans came back normal. Lee says his GP dismissed the idea of post-SSRI sexual dysfunction, even after being shown some academic papers. ‘If I’d gone blind, it would be obvious that something serious had happened,’ he says. ‘This is less obvious, but still has a huge impact. I’ve not had sex in three years.’
Other people contacting this newspaper include a 34-year-old woman who has spent 12 years unable to enjoy sex after being prescribed an antidepressant in her early 20s. ‘I’ve come to terms with the fact I might never experience sexual pleasure again,’ she says. Another man who developed the same symptoms after taking an SSRI earlier this year adds: ‘What I find particularly worrying is that this debilitating condition is not recognised by the medical establishment and that the wider public are not informed of the risks.
‘If I had known how profoundly the drug would affect my life, I would never have taken it.’
Professor of psychiatry David Healy, who set up the patient pressure group RxISK, has collected reports of PSSD from more than 1,000 patients, some of whom have suffered for at least 20 years. He says it appears to affect men and women equally, of any age, and regardless of the dose or duration of SSRI use.
‘While people with post-SSRI sexual dysfunction complain of lots of symptoms, including emotional numbness and brain fog, those can be caused by other things, like withdrawing from the drugs,’ he says.
‘The key to this is the genital numbness, which is quite distinctive – how do we explain why a few centimetres of tissue is affected?’
Theories about the cause involve serotonin, a chemical messenger in the brain that helps stabilise mood. Some people with depression are thought to have low levels of serotonin, and SSRIs work by boosting these levels. But too much could also be causing problems, some believe.
There may be interactions between serotonin and another brain chemical, dopamine, which helps us feel pleasure, or the drugs could trigger hormonal changes in the nervous system.
The MHRA is investigating whether the acne medication isotretinoin also leads to longer-term sexual dysfunction.
Luke Davidson, who set up the patient group UK PSSD Association, said officials at the regulator had told him they might look into post-SSRI sexual dysfunction, depending on the results of the isotretinoin investigation.
‘Lots more people have this than we realise, because many go on and off the drugs and are told their problems are linked to their depression and they don’t consider the drugs,’ he says.
Luke, who is 40 and from the South of England, has personal experience of PSSD. It was, he says, ‘like a switch had been flicked’ after taking citalopram during his 20s.
‘Something I’ve noticed on the forums is a lot of young adults saying they were put on SSRIs as children or teenagers and thought that they were asexual. It’s almost as if they never developed sexuality.’
One such teenager is Isabelle Jenkins. The 19-year-old student in Wales began taking an SSRI in 2019, when she was 16, and stopped in January. ‘I can tell if I’m being touched, but there’s no pleasure to the sensation,’ she says, tearfully.
‘People tell me it’s not important, but it is. I think about it every day. I wish I’d coped with my OCD without the drugs so I’d still have my sex life. It was a high price to pay.
‘I’m young, at university, and this should be the time of my life.’
There are concerns the rising tide of SSRI prescriptions, particularly since the pandemic, means there may be more cases of PSSD. More than 1.1 million prescriptions were given to teenagers last year, compared with 823,000 five years ago. Experts have also urged people prescribed SSRIs to not stop taking the medication without consulting their doctor.
Dr Moncrieff now hopes to gauge the prevalence of the problem by studying people who have come off SSRIs. ‘The terrible thing is it’s so hard to get this kind of research funded,’ she says. ‘There is endless research on new treatments but no one will fund research on worrying and potentially harmful effects of substances.’
As sufferer Rebecca Graham says: ‘If you tell your GP, “This SSRI is amazing, it’s changed my life”, they’ll believe you. If you say “This has ruined my life”, they tell you you’re wrong.
‘Can all of us really be wrong?’
susanne says
ADHD
Freedom of Information responses from the MHRA – week commencing 31 January 2022
Medicines & Healthcare products
Regulatory Agency
FOI release
Freedom of Information request on Risk Management Plan (RMP) approved for Melatonin Consilient Health 1 mg/ml oral solution (FOI 22/015)
Published 31 May 2022
FOI 22/015
3rd February 2022
Dear,……..
‘Thank you for your email, dated 5th January 2022, in which you requested:
“Risk Management Plan (RMP) approved for Melatonin Consilient Health 1 mg/ml oral solution”
We can confirm that the MHRA holds a copy of the requested RMP.
Information that has been redacted is exempt under Section 40 (Personal Information) or Section 43 (Commercial Interests) of the Freedom of Information (FOI) Act and is therefore withheld.
Section 40 provides that personal information may be exempt from release where to do so would contravene data protection principles. Section 43 provides that information will be exempt from release where to do so would or would be likely to prejudice commercial interests. Furthermore, we do not believe that there is an overriding public interest in disclosing the redacted information in this instance.’
AND snippetts Much more detailed info on their website
From Melatonin Consilient Health web site. (They also have an advert on this weeks’ thebmj)
recommended for ;-
– Insomnia in children and adolescents aged 6-17 years with ADHD, where sleep hygiene
measures have been insufficient
(Adults with jet lag
A maximum of 16 treatment cycles may occur per year.)
Paediatric population with ADHD
Recommended starting dose:
1-2 ml (equivalent to 1-2 mg) 30 to 60 minutes before bedtime.
The dose should be adjusted individually to a maximum of 5 ml (equivalent to 5 mg) daily regardless
of age.
Limited data are available for up to 3 years of treatment. After at least 3 months of treatment, the
physician should evaluate the treatment effect and consider stopping treatment if no clinically relevant
treatment effect is seen. The patient should be monitored at regular intervals (at least every 6 months)
to check that Melatonin is still the most appropriate treatment. During ongoing treatment, especially if
the treatment effect is uncertain, discontinuation attempts should be done regularly, e.g. once per year.
If the sleep disorder has started during treatment with medicinal products for ADHD, dose adjustment
or switching to another product should be considered.
Special populations
The effect of any degree of renal impairment on the pharmacokinetics of melatonin has not been
studied. .
There are no known studies on the use of melatonin in patients with hepatic impairment.
Children below 6 years of age
Melatonin Consilient Health is not recommended for children below 6 years with ADHD.
The capacity of the syringe is 5 ml with scale graduation of 0.2 ml.
Instruction for use
4.3 Contraindications
3
Hypersensitivity to the active substance or to any of the excipients listed in section
Possible long-term effects of melatonin have been inadequately studied.
There are theoretical risks
based on biological effects of melatonin, e.g. immunological regulation, effects on the threshold for
seizures and endocrinological effects, which could affect puberty development and fertility,
respectively.
Elderly
. It is unclear if significantly older persons are especially sensitive to exogenous melatonin.
Caution should therefore be exercised in treatment of this age group and individual dosage is
recommended.
Epilepsy
Caution when used in people with epilepsy, as melatonin has been reported to both increase and
decrease the frequency of seizures.
Immunological diseases
Occasional case reports have described exacerbation of an autoimmune disease in patients taking
melatonin.
There are no data regarding use of melatonin in patients with autoimmune diseases.
Melatonin Consilient Health is not recommended in patients with autoimmune diseases.
4.5 Interaction with other medicinal products and other forms of interaction
Interaction studies have only been performed in adults.
Whether these interactions are of clinical significance is unknown.
Fertility
There is limited clinical data about effects of melatonin on fertility. Animal studies
4.8 Undesirable effects
Melatonin causes few and no serious adverse reactions in the short term, up to three months. There is
limited documentation of long-term treatment with melatonin.
In the table below all adverse reactions are listed according to organ class and frequency: Very
common (≥1/10), Common (≥100, <1/10), Uncommon (≥1/1000, <1/100), Rare (≥1/10 000, <1/1000),
Very rare (<1/10 000), Not known (cannot be estimated from the available data).
Adverse reactions are presented within each frequency in order of decreasing seriousness.
Table 1
System organ class Frequency Adverse reaction
Infections and infestations Rare Herpes Zoster
Blood and lymphatic system
disorders
Rare Leukopenia, thrombocytopenia
Immune system disorders Not known Hypersensitivity reaction
Metabolism and nutrition
disorders
Rare Hypertriglyceridaemia,
hypocalcaemia, hyponatraemia
Psychiatric disorders Uncommon Irritability, nervousness,
restlessness, insomnia,
abnormal dreams, nightmares,
anxiety
Rare Mood altered, aggression,
agitation, crying, stress
symptoms, disorientation, early
morning awakening, libido
increased, depressed mood,
depression
Nervous system disorders Common Headache, somnolence
6
Uncommon Migraine, lethargy,
psychomotor hyperactivity,
dizziness
Rare Syncope, memory impairment,
disturbance in attention, dreamy
state, restless legs syndrome,
poor quality sleep, paraesthesia
Eyes Rare Visual acuity reduced,
vision blurred, lacrimation
increased
Ear and labyrinth disorders Rare Vertigo positional, vertigo
Cardiac disorders Rare Angina pectoris, palpitations
Vascular disorders Uncommon Hypertension
Rare Hot flush
Gastrointestinal disorders Uncommon Abdominal pain, abdominal
pain upper, dyspepsia, mouth
ulceration, dry mouth, nausea
Rare Gastro-esophageal reflux
disease, gastrointestinal
disorder, oral mucosal
blistering, tongue ulceration,
gastrointestinal upset, vomiting,
bowel sounds abnormal,
flatulence, salivary
hypersecretion, halitosis,
abdominal discomfort, gastric
disorder, gastritis
Hepatobiliary disorders Uncommon Hyperbilirubinaemia
Skin and subcutaneous tissue
disorders
Uncommon Dermatitis, night sweats,
pruritus, rash, pruritus
generalised, dry skin
Rare Eczema, erythema, hand
dermatitis, psoriasis, rash
generalised, rash pruritic, nail
disorder
Not known Angioedema, oedema of
mouth, tongue oedema
Musculoskeletal and
connective tissue disorders
Uncommon Pain in extremity
Rare Arthritis, muscle spasms, neck
pain, night cramps
Renal and urinary disorders Uncommon Glycosuria, proteinuria
Rare Polyuria, haematuria, nocturia
Reproductive system and
breast disorders
Uncommon Menopausal symptoms
Rare Priapism, prostatitis
Not known Galactorrhea
General disorders and
administration site conditions
Uncommon Asthenia, chest pain
Rare Fatigue, pain, thirst
Investigations Uncommon Liver function test abnormal,
weight increased
Rare Hepatic enzyme increased,
blood electrolytes abnormal,
laboratory test abnormal
Pediatric population
In the pediatric population a low frequency of generally mild adverse reactions has been reported. The
adverse events have not been significantly different in children who has received placebo compared to
7
children who received melatonin. The most common adverse effects were headache, hyperactivity,
vertigo and abdominal pain. No serious adverse effects have been observed.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It
allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare
professionals are asked to report any suspected adverse reactions via Yellow Card Scheme, website:
http://www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App
Store.
4.9 Overdose
Administration of repeated daily doses of up to 300 mg melatonin without any clinically significant
side effects has been reported in the literature.
Drowsiness can be expected in case of overdose. Due to the short half-life of melatonin, complete
elimination of melatonin from the body is expected within 12 hours of ingestion. Physicians should
assess whether common overdose measures should be used.
5. PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Psychoeleptics, melatonin receptor agonists, ATC code: N05CH01.
Melatonin (N-acetyl-5-methoxytryptamine) is an endogenous hormone produced by the epiphysis and
structurally related to serotonin. Melatonin is involved in controlling the circadian rhythm and
adaptation to the light-dark cycle. It is also associated with a sedative effect and an increased
propensity for sleep.
Serum concentrations of endogenous melatonin vary over the day. Melatonin levels increase during
the dark hours of the day with maximum serum concentrations between 02 and 04 in the morning
(Srinivasan 2009; Tordjman 2017). Thereafter, serum levels of melatonin gradually decrease. Only a
small amount of melatonin is excreted during the light hours of the day.
Mechanism of action
The activity of melatonin on MT1, MT2 and MT3 receptors is thought to contribute to its sleeppromoting properties since these receptors (especially MT1 and MT2) are involved in the regulation of
diurnal rhythm and sleep regulation.
Pharmacodynamic effects
Melatonin has a hypnotic / sedative effect and increases propensity for sleep. Melatonin administered
earlier or later than the nocturnal peak in melatonin secretion can, respectively, advance or delay the
circadian rhythmicity of melatonin secretion. Administration of melatonin at bedtime (between 22:00
and 24:00 hr) at destination following rapid transmeridian travel (aircraft flight) hastens
resynchronisation of circadian rhythmicity from 'departure time' to 'destination time', and ameliorates
the collection of symptoms known as jet lag that are a consequence of such de-synchronisation.
Clinical efficacy and safety
melatonin effectively
humans.
Paediatric population
Melatonin treatment has been studied in a 4-week randomized, double-blind, placebo-controlled study
conducted in 105 children between 6-12 years of age, with ADHD and chronic sleep onset insomnia
(van der Heijden KB et al. 2007). Participants received melatonin (3 mg when body weight 40 kg [n = 9]) in fast-release tablets or placebo.
Mean actigraphic estimate of sleep onset advanced by 26.9 ± 47.8 minutes with melatonin, whereas
there was a delay of 10.5 ± 37.4 minutes with placebo (p 30 minutes compared to 12.8% with placebo (p =
0.001). There was an increase in mean total time asleep of 19.8 ± 61.9 minutes with melatonin and a
decrease of 13.6 ± 50.6 minutes with placebo (p = 0.01). As compared with placebo, the melatonin
group showed a decrease in sleep latency (p = 0.001) and increase in sleep efficiency (p = 0.01). The
mean score on sleep log item difficulty falling asleep decreased by 1.2 ± 1.3 points (35.3% of
baseline) with melatonin and by 0.1 ± 0.8 points (4.3% of baseline) with placebo (p < 0.0001).
There was no significant effect on behaviour, cognition, and quality of life. There were no
discontinuations or withdrawals caused by adverse events.
The effect of renal impairment on the pharmacokinetics of melatonin administered has not been
studied.
5.3 Preclinical safety data
Current studies on safety pharmacology, general toxicity, genotoxicity and carcinogenicity, did not
show any particular risks to humans.
7. MARKETING AUTHORISATION HOLDER
Consilient Health Ltd.,
8. MARKETING AUTHORISATION NUMBER(S)
PL 24837/0133
10. DATE OF REVISION OF THE TEXT
02/2022
susanne says
ADHD etc According to this – well it does – but it doesn’t – or it doesn’t but it does.
JAMA Intern Med. Published online October 3, 2022. doi:10.1001/jamainternmed.2022.4268
Question Is antidepressant exposure during pregnancy associated with an increased risk of specific neurodevelopmental disorders in children?
Findings In this cohort study including 145 702 antidepressant-exposed pregnancies, antidepressant exposure during pregnancy was not associated with autism spectrum disorder, attention-deficit/hyperactivity disorder, specific learning disorders, developmental speech/language disorders, developmental coordination disorders, intellectual disabilities, or behavioral disorders after accounting for confounding through various design and analytic approaches. Results were generally consistent across antidepressant medication classes, commonly used individual drugs, and gestational exposure windows.
In contrast with the present null results for ASD, an analysis of Swedish mother-child pairs reported an association between citalopram and escitalopram use and ASD, but not with other selective serotonin reuptake inhibitors.24 Further investigation of the association with escitalopram may be warranted.Meaning These findings suggest that antidepressant use in pregnancy does not increase the risk of neurodevelopmental disorders in children.
Conclusions
Results of this cohort study suggest that antidepressant use in pregnancy does not increase the risk of NDDs in children. However, elevated crude cumulative incidence estimates for NDDs suggest that antidepressant use by pregnant individuals is a robust marker of NDD risk in children. Therefore, antidepressant exposure during pregnancy could be an important marker for early screening and intervention in children, with the goal of improving outcomes for NDDs.
Or on Pulse Today
Home News Clinical areas Mental health and addiction Antidepressants in pregnancy not linked to autism, finds large study
03 October 2022
Antidepressant use in pregnancy does not in itself increase the risk of neurodevelopmental disorders such as autism in children, a large study has found.
But women using antidepressants during pregnancy did have a higher risk of having a child with a neurodevelopmental disorder than individuals not using antidepressants, suggesting factors other than the medication may be involved.
Previous studies that have looked at this issue, most of which have focused on autism and attention deficit hyperactivity disorder (ADHD) have produced conflicting results and the issue remains controversial, the researchers reported in JAMA Internal Medicine.
A team at Harvard Medical School looked at 3.2 million pregnancies across two large health insurance databases with children followed for up to 14 years.
The crude results from 145,702 pregnancies with antidepressant exposure and more than 3 million unexposed pregnancies showed a doubling in risk of a range of neurodevelopmental outcomes.
But once the team had adjusted the analyses for an ‘extensive list’ of potential confounding factors this association began to drop away, they reported.
Overall individuals exposed to antidepressants were older and had greater medication use during pregnancy than unexposed individuals and in one of the databases, antidepressant- exposed individuals were also more likely to be white.
Careful comparisons with women who had discontinued antidepressants before pregnancy further shifted the risk towards zero and when they looked at exposed and non-exposed siblings there was no increased risk of antidepressant use.
Autism has been the most studied neurodevelopmental disorder related to antidepressants in pregnancy with some reports of 20-80% increased risk.
But after adjusting the findings for a broad range of factors, there was no association in their analysis, the researchers said.
Yet the crude association they found suggests that antidepressant use during pregnancy may be a ‘robust marker’ for neurodevelopmental risk in children and could be useful for early screening and intervention in children.
Professor Carmine Pariante, professor of biological psychiatry at the Institute of Psychiatry, Psychology and Neuroscience, King’s College London, said this was ‘truly an important paper’.
‘What this study shows is that, in reality, previous concerns that antidepressant use increases the risk of autism or other neurodevelopmental disorders are due to the effects of depression itself, or to risk factors for depression, and not to antidepressants.
‘Women with clinically significant depression, or other mental disorders where antidepressants are indicated, should be informed that the risk associated with antidepressants use in pregnancy is not as high as previously thought, and should be offered the possibility to discuss this therapeutic option as part of a package of care that should include also psychological and social support.’
Patrick D Hahn says
I checked the database. There were thirty hits for “amphetamine” but only two were adverse event reports — one sixty-seven-year-old woman, and one sixty-seven-year-old man.
No hits for “methylphenidate.”
Let’s keep asking questions,
Dr. David Healy says
Patrick
37 for amphetamine is fascinating. This is a big increase on just putting in ADHD. To get the real picture you might have to put in dexamphetamine, lisdexamphetamine, Vyvanse, Focalin etc along with dex-methlylphenidate etc and of course atomoxetine
These are likely US only and the contrast to the Rest of World will be interesting
David
Perhotelan says
Many report they no longer experience sexual or romantic attraction at all, and have been left with an emotional numbness