What is PSSD?
Post-SSRI sexual dysfunction (PSSD) is an iatrogenic condition in which sexual function does not return to normal after the discontinuation of serotonin reuptake inhibiting antidepressants.1 This group includes:
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin-norepinephrine reuptake inhibitors (SNRIs)
- some tricyclic antidepressants such as clomipramine and imipramine
Commonly used SSRIs include:
- paroxetine (Paxil, Seroxat)
- fluoxetine
- sertraline (Zoloft)
- citalopram (Celexa)
- escitalopram (Lexapro)
- vortioxetine (Trintellix)
Common SNRIs include:
- venlafaxine (Effexor)
- desvenlafaxine (Pristiq)
- duloxetine
Most people who take an SSRI or related medication will feel some degree of genital numbing, often within 30 minutes of taking the first dose. In PSSD, this genital numbing and other sexual side effects remain or do not resolve completely when the drug is stopped. In some cases, a mild dysfunction while on the medication can get worse upon stopping or reducing the dose.2
PSSD affects both men and women. It can happen after only a few days of using an antidepressant and can persist indefinitely. There is no known cure.
Some healthy volunteers had persistent sexual dysfunction after stopping SSRIs in unpublished phase 1 trials in the 1980s.3 The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) received their first report of a persistent sexual dysfunction after stopping an SSRI in 1991.4 Post-SSRI sexual dysfunction first appeared in the peer-reviewed medical literature in 2006.5, 6 See our list of PSSD Literature.
PSSD can be extremely distressing and lead to marriage break-up and job loss. There have also been confirmed suicides.
Symptoms of PSSD
Symptoms of PSSD can include:
- reduced genital sensation
- decreased libido
- erectile dysfunction/decreased vaginal lubrication
- pleasureless or weak orgasm
- difficulty achieving orgasm
- reduced response to sexual stimuli
- decreased or loss of nocturnal erections
- reduced nipple sensitivity
- flaccid glans during erection
Genital numbness and pleasureless orgasm are characteristic features of PSSD and help to separate it from other types of sexual dysfunction. Depression and other mental health disorders do not cause these symptoms.
You may notice a reduction in tactile sensation (genitals feel like they were exposed to an anesthetic), or you may be more aware of a reduction in sexual sensation (genital touch feels little different to being touched on a non-sexual body part). Or you might notice a combination of both.
Orgasm is experienced with little or no sensation of pleasure. Men can also have reduced ejaculatory force.
Cases of premature ejaculation after stopping an SSRI have also been reported.7
Some women experience reduced vaginal lubrication, but this may not occur in all cases.8
People with PSSD often report non-sexual symptoms such as emotional numbing and cognitive impairment. However, these and other symptoms can be present without PSSD. They are therefore best regarded as accompanying symptoms rather than being part of the condition itself.
The severity of symptoms can vary in different people. If your sexual function is not the same as before using antidepressants, you may be suffering from PSSD.
How is PSSD diagnosed?
PSSD is diagnosed by considering several factors including medication history, onset and profile of the symptoms, and by eliminating other possible causes.
Diagnostic criteria for PSSD were published in 2021.9
Necessary
(1) Prior treatment with a serotonin reuptake inhibitor.
(2) An enduring change in somatic (tactile) or erogenous (sexual) genital sensation after treatment stops.
Additional
(3) Enduring reduction or loss of sexual desire.
(4) Enduring erectile dysfunction (males).
(5) Enduring inability to orgasm or decreased sensation of pleasure during orgasm.
(6) The problem is present for ≥3 months after stopping treatment.
There should be
(7) No evidence of pre-drug sexual dysfunction that matches the current profile.
(8) No current medical conditions that could account for the symptoms.
(9) No current medication or substance misuse that could account for the symptoms.
PSSD is often misdiagnosed as a psychological problem when it is actually pharmacological in origin.10
Quantitative sensory testing (QST) of the penis routinely detects reduced sensitivity in male PSSD patients, but it’s not a widely available test.11
PSSD can sometimes result in borderline testosterone or other hormones. However, testosterone treatment has not been shown to benefit the condition.
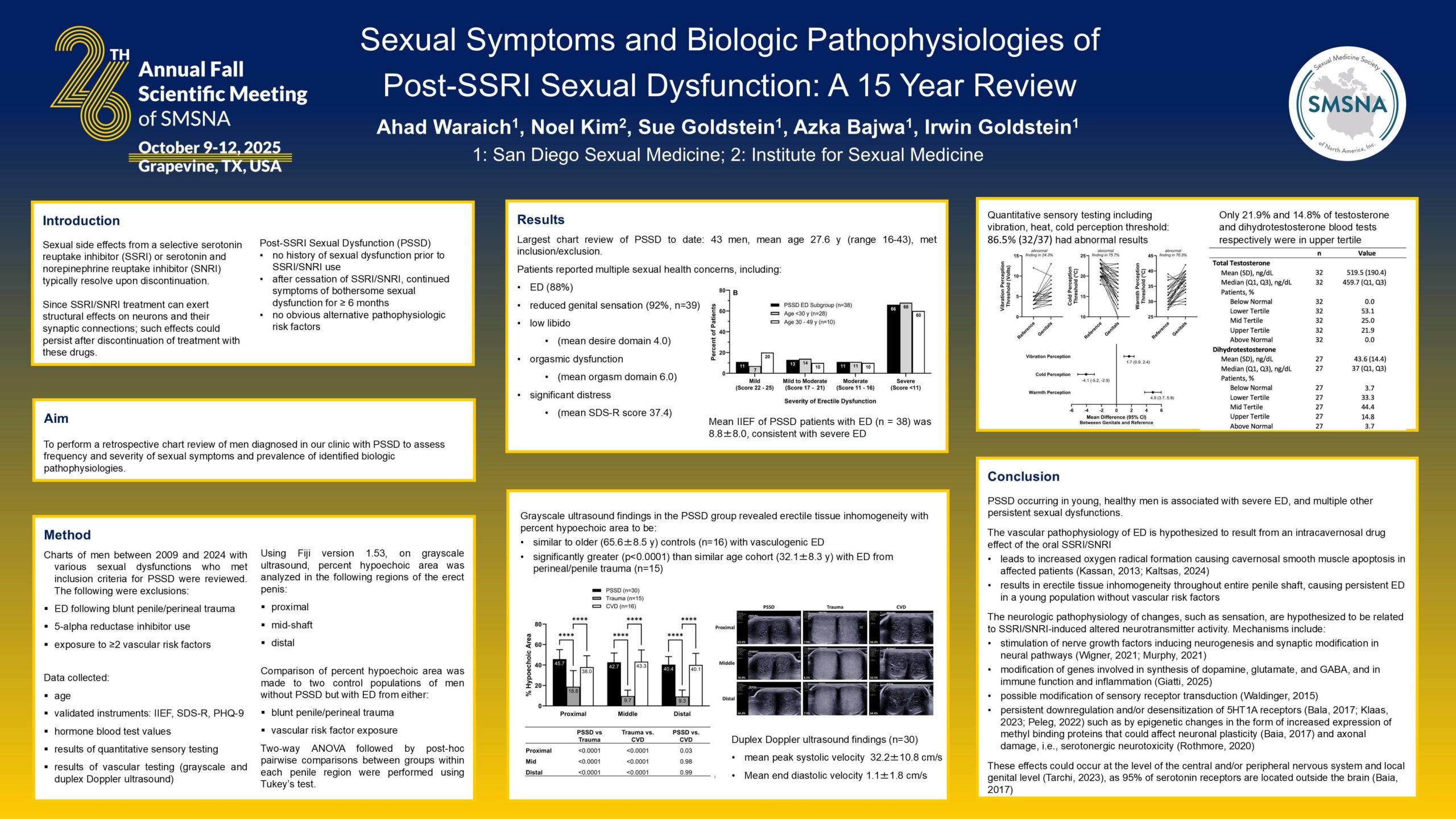
There is some evidence that PSSD may lead to damage of erectile tissue in men. These findings from a 15 year review were presented at an academic meeting in October 2025, but are yet to be published in a peer-reviewed journal.12
In 2024, post-SSRI sexual dysfunction was added to SNOMED CT, an international set of clinical healthcare terminology for use in electronic health records. This means that PSSD can now be more formally recorded in medical records by using the code SCTID 1340196008.
How common is PSSD?
There are no reliable estimates of the incidence and prevalence of PSSD. It is not known how many people, if any, fully regain their original sexual function and sensation after using an antidepressant. Based on the available data, PSSD may be quite common.
In one study, a group of patients who all had sexual side effects on an SSRI were switched to another drug called amineptine, which was found to have no sexual side effects. Six months later, 55% of those who had previously been on an SSRI still had sexual dysfunction.13
A large placebo-controlled study into the use of sertraline as a treatment for premature ejaculation found that the ejaculation-delaying effect of the drug persisted for 34% of participants 6 months after it was discontinued.14
A healthy volunteer study of paroxetine reported that erectile and ejaculatory functions had not returned to baseline four weeks after discontinuation of the drug, with 9% of patients complaining of more than mild dysfunction.15
A 2024 review article described many factors that can lead to under-reporting and under-recognition of PSSD.16 These included patient embarrassment at raising sexual concerns, unhelpful responses from healthcare providers, and patient unawareness that their sexual difficulties are linked to prior medication. See Post-SSRI sexual dysfunction: barriers to quantifying incidence and prevalence.
Also in 2024, a US/Canada survey of sexual and gender minority youth aged 15 to 29 reported that 13.2% of patients treated with antidepressants had a persistent post-treatment genital hypoesthesia compared to 0.9% of those treated with other medications.17
Can PSSD be prevented?
It is not possible to determine who will develop PSSD when an antidepressant is stopped, or any way to actively prevent it. Reducing the dose gradually (tapering) does not appear to prevent the condition. There is no evidence that adding another drug to an antidepressant to combat sexual side effects (eg. bupropion) will prevent PSSD when the antidepressant is stopped.
There is no evidence for any precipitating factors other than the use of a serotonin reuptake inhibitor. Psychological stress does not contribute to the risk of developing PSSD.
Potential risks in pregnancy
There may be long-term sexual consequences for offspring exposed to antidepressants during pregnancy or at a young age.
Rodent studies have shown that treatment with SSRIs at a young age resulted in permanently decreased sexual behavior in adulthood, with the presence of long-term neurological changes.18, 19, 20 Maternal exposure to fluoxetine also impaired sexual motivation in adult male mice.21
A systematic review of the literature on persistent sexual dysfunction in animals after early exposure to SSRIs concluded: “Our results showed substantial and lasting effects on sexual behaviour in rats after exposure to an SSRI early in life on important sexual outcomes.”22
It is not known whether PSSD can be inherited from a parent with the condition in the absence of prenatal exposure. Although it did not involve PSSD, a study of zebrafish found that behavioural changes from exposure to fluoxetine persisted for three subsequent generations of unexposed decedents.23
Fluoxetine has been classified as a reproductive toxin by the Center for the Evaluation of Risks to Human Reproduction (CERHR), an expert panel at the National Institute of Environmental Health Sciences, part of the National Institutes of Health.24
Warnings in medication labels
Since 2011, the US Prozac patient information sheet has warned: “Symptoms of sexual dysfunction occasionally persist after discontinuation of fluoxetine treatment”.25
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) states: “In some cases, serotonin reuptake inhibitor-induced sexual dysfunction may persist after the agent is discontinued”.26
In response to a petition and adverse event data from RxISK in 2018, the European Medicines Agency recommended changes to SSRI and SNRI product labels to include information about persistent sexual dysfunction after stopping the medication.27, 28
We also submitted the petition to the US Food and Drug Administration (FDA) with an offer to supply details of patients who were willing to be contacted. Other than two standard acknowledgement letters, there has been no further response.29
Medication labels have since been updated in Ireland, New Zealand, Canada, Hong Kong, Australia and Malaysia.30, 31
What causes PSSD?
It is not known how serotonin reuptake inhibitors cause PSSD. Several hypotheses have been proposed including serotonergic neurotoxicity, epigenetic alternations, and disturbances in transient receptor potential ion channels.32, 33
Treatment with fluoxetine has been shown to cause persistent desensitization of 5-HT1A receptors after removal of the SSRI in rats.34 In another study, a 5-HT1A antagonist was shown to reverse and prevent sexual dysfunction in rats that were being administered with fluoxetine.35 However, attempts by PSSD patients to manipulate the serotonergic and dopaminergic systems in an effort to resolve the condition have been unsuccessful.
Animal studies have shown changes in bioelectric cell properties and neuroactive steroids after withdrawal of an SSRI.36, 37
In 2022, a group of Finnish PSSD patients reported that they had tested positive for low nerve fibre density, suggesting possible small fibre neuropathy.38
SSRI side effects include impaired semen quality and damage to sperm DNA39, 40, 41, 42 as well as issues that are often linked to the endocrine system such as hormone imbalances43, 44 and breast enlargement.45 SSRIs have also been found to have effects on sex steroids.46 However, it is unclear whether PSSD involves endocrine disruption.
Is there any treatment for PSSD?
There is currently no treatment for PSSD. A number of medications and supplements can produce positive sexual effects in some sufferers.47 However, these can come with their own risks, and the results are generally very limited and inconsistent.
PDE5 inhibitors (eg. sildenafil and tadalafil) often have reduced effectiveness in people with PSSD, and they have no direct effect on the loss of sensation.48, 49 Vortioxetine is not a treatment for PSSD and has been linked to the onset or worsening of the condition.50 Psychosexual counselling, cognitive-behavioural therapy and lifestyle changes such as exercise and dietary improvements do not benefit the condition.
One patient regained a moderate degree of penile sensitivity following treatment with low-power laser irradiation, but there was no improvement in sexual responsiveness.51
Some people have reported an improvement over time, but many fail to recover to any significant degree. Some have had the condition for over 20 years without any improvement.
If you are suffering from PSSD, you might have difficulty finding professional support for your condition, as healthcare providers are often reluctant to engage with serious problems caused by medications. If you are having difficulty finding someone in your country, we have a small list of doctors who are a familiar with PSSD.
Our PSSD Research Fund was launched in 2022, and our RxISK Prize of $100,000 USD is offered to anyone who can provide a cure.
Reporting your condition
If you are suffering from PSSD, you can report it to us by completing a RxISK Report. Please provide as much detail as possible including the dates that you started and stopped the drug.
You might also want to report your condition to your country’s drug regulator such as MedWatch in the US and the Yellow Card Scheme in the UK.
Drug regulators use codes from the Medical Dictionary for Regulatory Activities (MedDRA) when logging reports. MedDRA introduced a code for post-SSRI sexual dysfunction (10086208) in 2021. When reporting, you should mention this code in addition to providing details of your symptoms.
As of 2025, UK and German regulators have confirmed that they are using the MedDRA code for PSSD and have received 95 and 39 reports, respectively. Regulators do not usually reclassify previous reports when a new code is introduced, so any previous reports are unlikely to be coded as PSSD unless submitted again.
Media coverage
For many years, the media was reluctant to cover PSSD, claiming they did not want to stop people from taking their antidepressants. Media coverage has only improved in recent years due to an increasing number of publications about the condition in medical journals and the introduction of warnings in medication labels. See PSSD in the Media.
Other drugs and conditions
Other medications that may cause persistent sexual side effects after stopping the drug include:
- Antihistamines that are serotonin reuptake inhibiting
- Ziprasidone – an antipsychotic that is also a serotonin reuptake inhibitor
- Some antibiotics that may be serotonin reuptake inhibiting such as tetracycline and doxycycline
- FDA updated the product information for finasteride products in 2011 to warn of persisting sexual side effects after discontinuation of treatment, with further warnings added in 2012.52
- Isotretinoin (Accutane) is a treatment for acne and is also serotonin reuptake inhibiting53
The use of SSRIs or SNRIs, and often their withdrawal, has consistently been reported as one of the triggers of persistent genital arousal disorder (PGAD). This is essentially the opposite of PSSD, causing a relentless sense of arousal and discomfort in the genitals, but without any accompanying feeling of desire.54
References
- Healy D, Le Noury J, Mangin D. Enduring sexual dysfunction after treatment with antidepressants, 5α-reductase inhibitors and isotretinoin: 300 cases. Int J Risk Saf Med. 2018;29(3-4):125-134. PMID: 29733030. ↩︎
- Bala A, Tue Nguyen HM, Hellstrom WJG. Post-SSRI Sexual Dysfunction: A Literature Review. Sex Med Rev. 2018;6(1):29-34. PMID: 28778697. ↩︎
- Healy D. Antidepressants and sexual dysfunction: a history. J R Soc Med. 2020;113(4):133-135. Epub 2020 Jan 23. PMID: 31972096. ↩︎
- Email from MHRA to K Bennett, 23 May 2019. ↩︎
- Csoka AB, Shipko S. Persistent sexual side effects after SSRI discontinuation. Psychother Psychosom. 2006;75(3):187-8. PMID: 16636635. ↩︎
- Bahrick AS. Post SSRI sexual dysfunction. ASAP Tablet. 2006;7(3):2-3,10-11. ↩︎
- Adson DE, Kotlyar M. Premature ejaculation associated with citalopram withdrawal. Ann Pharmacother. 2003;37(12):1804-6. PMID: 14632589. ↩︎
- Patacchini A, Cosci F. Exposure to serotonin selective reuptake inhibitors or serotonin noradrenaline reuptake inhibitors and sexual dysfunction: Results from an online survey. Int J Risk Saf Med. 2021;32(3):229-242. PMID: 33579876. ↩︎
- Healy D, Bahrick A, Bak M, Barbato A, Calabrò RS, Chubak BM, et al. Diagnostic criteria for enduring sexual dysfunction after treatment with antidepressants, finasteride and isotretinoin. Int J Risk Saf Med. 2022;33(1):65-76. PMID: 34719438. ↩︎
- Healy D, Le Noury J, Mangin D. Post-SSRI sexual dysfunction: Patient experiences of engagement with healthcare professionals. Int J Risk Saf Med. 2019;30(3):167-178. PMID: 31450514. ↩︎
- Waraich A, Clemons C, Ramirez R, Yih J, Goldstein S, Goldstein I. Post-SSRI sexual dysfunction (PSSD): Ten year retrospective chart review. J Urol. 2020;203(4):e1179. ↩︎
- Waraich A, Kim N, Goldstein S, Bajwa A, Goldstein I. Sexual symptoms and biologic pathophysiologies of post-SSRI sexual dysfunction: A 15 year review. 26th Annual Fall Scientific Meeting of SMSNA. 9-12 October 2025. ↩︎
- Montejo AL, Llorca G, Izquierdo JA, Carrasco JL, Daniel E, Pérez-Sola V, et al. Sexual dysfunction with antidepressive agents. Effect of the change to amineptine in patients with sexual dysfunction secondary to SSRI. Actas Esp Psiquiatr (in Spanish). 1999;27(1):23-34. PMID: 10380144. ↩︎
- Arafa M, Shamloul R. Efficacy of sertraline hydrochloride in treatment of premature ejaculation: a placebo-controlled study using a validated questionnaire. Int J Impot Res. 2006;18(6):534-8. Epub 2006 Mar 23. PMID: 16554853. ↩︎
- Tanrikut C, Feldman AS, Altemus M, Paduch DA, Schlegel PN. Adverse effect of paroxetine on sperm. Fertil Steril. 2010;94(3):1021-6. Epub 2009 Jun 10. PMID: 19515367. ↩︎
- Healy D, Mangin D. Post-SSRI sexual dysfunction: barriers to quantifying incidence and prevalence. Epidemiol Psychiatr Sci. 2024 Sep 18;33:e40. PMID: 39289881. ↩︎
- Pirani Y, Delgado-Ron JA, Marinho P, Gupta A, Grey E, Watt S, MacKinnon KR, Salway T. Frequency of self-reported persistent post-treatment genital hypoesthesia among past antidepressant users: a cross-sectional survey of sexual and gender minority youth in Canada and the US. Soc Psychiatry Psychiatr Epidemiol. 2024 Sep 20. Epub ahead of print. PMID: 39302425. ↩︎
- Maciag D, Simpson KL, Coppinger D, Lu Y, Wang Y, Lin RC, et al. Neonatal Antidepressant Exposure has Lasting Effects on Behavior and Serotonin Circuitry. Neuropsychopharmacology. 2006;31(1):47-57. PMID: 16012532. ↩︎
- de Jong TR, Snaphaan LJ, Pattij T, Veening JG, Waldinger MD, Cools AR, et al. Effects of chronic treatment with fluvoxamine and paroxetine during adolescence on serotonin-related behavior in adult male rats. Eur Neuropsychopharmacol 2006;16(1):39-48. PMID: 16107310. ↩︎
- Iñiguez SD, Warren BL, Bolaños-Guzmán CA. Short- and long-term functional consequences of fluoxetine exposure during adolescence in male rats. Biol Psychiatry. 2010;67(11):1057-66. PMID: 20172503. ↩︎
- Gouvêa TS, Morimoto HK, de Faria MJ, Moreira EG, Gerardin DC. Maternal exposure to the antidepressant fluoxetine impairs sexual motivation in adult male mice. Pharmacol Biochem Behav. 2008;90(3):416-9. PMID: 18457868. ↩︎
- Simonsen AL, Danborg PB, Gøtzsche PC. Persistent sexual dysfunction after early exposure to SSRIs: Systematic review of animal studies. Int J Risk Saf Med. 2016;28(1):1-12. PMID: 27176752. ↩︎
- Vera-Chang MN, St-Jacques AD, Gagné R, Martyniuk CJ, Yauk CL, Moon TW, Trudeau VL. Transgenerational hypocortisolism and behavioral disruption are induced by the antidepressant fluoxetine in male zebrafish Danio rerio. Proc Natl Acad Sci U S A. 2018;115(52):E12435-E12442. Epub 2018 Dec 10. PMID: 30530669. ↩︎
- Hines RN, Adams J, Buck GM, Faber W, Holson JF, Jacobson SW, et al. NTP-CERHR Expert Panel Report on the reproductive and developmental toxicity of fluoxetine. Birth Defects Res B Dev Reprod Toxicol. 2004;71(4):193-280. PMID: 15334524. ↩︎
- US Prozac product information at https://pi.lilly.com/us/prozac.pdf. ↩︎
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). American Psychiatric Association, 2013. Page 449. ↩︎
- Healy D. Citizen petition: Sexual side effects of SSRIs and SNRIs. Int J Risk Saf Med. 2018;29(3-4):135-147. PMID: 29733031. ↩︎
- European Medicines Agency. PRAC recommendations on signals adopted at the 13-16 May 2019 PRAC meeting. Published June 11, 2019. Page 5. ↩︎
- Citizen petition at https://www.regulations.gov/document/FDA-2018-P-1846-0001. ↩︎
- Therapeutic Goods Administration. Updated warnings about persistent sexual dysfunction for antidepressants. 23 May 2024. https://www.tga.gov.au/news/safety-updates/updated-warnings-about-persistent-sexual-dysfunction-antidepressants. ↩︎
- National Pharmaceutical Regulatory Agency (NPRA). Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs): Risk of Persistent Sexual Dysfunction. 14 November 2025. ↩︎
- Ben-Sheetrit J, Aizenberg D, Csoka AB, Weizman A, Hermesh H. Post-SSRI Sexual Dysfunction: Clinical Characterization and Preliminary Assessment of Contributory Factors and Dose-Response Relationship. J Clin Psychopharmacol. 2015;35(3):273-8. PMID: 25815755. ↩︎
- Klaas S, Siva JB, Bak M, Govers M, Schreiber R. The pathophysiology of Post SSRI Sexual Dysfunction – Lessons from a case study. Biomed Pharmacother. 2023;161:114166. Epub 2023 Mar 8. PMID: 36898260. ↩︎
- Raap DK, Garcia F, Muma NA, Wolf WA, Battaglia G, van de Kar LD. Sustained desensitization of hypothalamic 5-Hydroxytryptamine1A receptors after discontinuation of fluoxetine: inhibited neuroendocrine responses to 8-hydroxy-2-(Dipropylamino)Tetralin in the absence of changes in Gi/o/z proteins. J Pharmacol Exp Ther. 1999;288(2):561-7. PMID: 9918559. ↩︎
- Sukoff Rizzo SJ, Pulicicchio C, Malberg JE, Andree TH, Stack GP, Hughes ZA, et al. 5-HT(1A) receptor antagonism reverses and prevents fluoxetine-induced sexual dysfunction in rats. Int J Neuropsychopharmacol. 2009;12(8):1045-53. PMID: 19435548. ↩︎
- Healy D, LaPalme J, Levin M. Post-SSRI Sexual Dysfunction: A Bioelectric Mechanism? Bioelectricity. 2020;2(1):7-13. Epub 2020 Mar 18. PMID: 34471832; PMCID: PMC8370302. ↩︎
- Giatti S, Diviccaro S, Cioffi L, Falvo E, Caruso D, Melcangi RC. Effects of paroxetine treatment and its withdrawal on neurosteroidogenesis. Psychoneuroendocrinology. 2021;132:105364. PMID: 34325207. ↩︎
- Blog post: Sensory Receptors, Small Fibres and Neuropathy. ↩︎
- Tanrikut C, Schlegel PN. Antidepressant-associated changes in semen parameters. Urology. 2007;69(1):185.e5-7. PMID: 17270655. ↩︎
- Safarinejad MR. Sperm DNA damage and semen quality impairment after treatment with selective serotonin reuptake inhibitors detected using semen analysis and sperm chromatin structure assay. J Urol. 2008;180(5):2124-8. PMID: 18804223. ↩︎
- Koyuncu H, Serefoglu EC, Yencilek E, Atalay H, Akbas NB, Sarıca K. Escitalopram treatment for premature ejaculation has a negative effect on semen parameters. Int J Impot Res. 2011;23(6):257-61. PMID: 21776003. ↩︎
- Akasheh G, Sirati L, Noshad Kamran AR, Sepehrmanesh Z. Comparison of the effect of sertraline with behavioral therapy on semen parameters in men with primary premature ejaculation. Urology. 2014;83(4):800-4. PMID: 24529582. ↩︎
- Safarinejad MR. Evaluation of endocrine profile and hypothalamic-pituitary-testis axis in selective serotonin reuptake inhibitor-induced male sexual dysfunction. J Clin Psychopharmacol. 2008;28(4):418-23. PMID: 18626269. ↩︎
- Cohen AJ. Antidepressant-Induced Sexual Dysfunction Associated With Low Serum Free Testosterone. Psychiatry Online. 1999. ↩︎
- Amsterdam JD, Garcia-España F, Goodman D, Hooper M, Hornig-Rohan M. Breast enlargement during chronic antidepressant therapy. J Affect Disord. 1997;46(2):151-6. PMID: 9479619. ↩︎
- Jacobsen NW, Hansen CH, Nellemann C, Styrishave B, Halling-Sørensen B. Effects of selective serotonin reuptake inhibitors on three sex steroids in two versions of the aromatase enzyme inhibition assay and in the H295R cell assay. Toxicol In Vitro. 2015;29(7):1729-35. PMID: 26162595. ↩︎
- Calabrò RS, De Luca R, Manuli A, Portaro S, Naro A, Quattrini F. Towards Improving Post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons from a Case Study. J Sex Marital Ther. 2019;45(6):562-565. Epub 2019 Feb 13. PMID: 30640584. ↩︎
- Reisman Y. Post-SSRI sexual dysfunction. BMJ. 2020;368:m754. PMID: 32107204. ↩︎
- Csoka AB, Bahrick A, Mehtonen OP. Persistent sexual dysfunction after discontinuation of selective serotonin reuptake inhibitors. J Sex Med. 2008;5(1):227-33. PMID: 18173768. ↩︎
- Studt A, Gannon M, Orzel J, Vaughan A, Pearlman AM. Characterizing post-SSRI sexual dysfunction and its impact on quality of life through an international online survey. Int J Risk Saf Med. 2021;32(4):321-329. PMID: 34366299. ↩︎
- Waldinger MD, van Coevorden RS, Schweitzer DH, Georgiadis J. Penile anesthesia in Post SSRI Sexual Dysfunction (PSSD) responds to low-power laser irradiation: a case study and hypothesis about the role of transient receptor potential (TRP) ion channels. Eur J Pharmacol. 2015;753:263-8. PMID: 25483212. ↩︎
- FDA. Questions and Answers: Finasteride Label Changes. ↩︎
- Healy D. Post-SSRI sexual dysfunction & other enduring sexual dysfunctions. Epidemiol Psychiatr Sci. 2019;29:e55. PMID: 31543091. ↩︎
- Goldstein I, Komisaruk BR, Pukall CF, Kim NN, Goldstein AT, Goldstein SW, Hartzell-Cushanick R, Kellogg-Spadt S, Kim CW, Jackowich RA, Parish SJ, Patterson A, Peters KM, Pfaus JG. International Society for the Study of Women’s Sexual Health (ISSWSH) Review of Epidemiology and Pathophysiology, and a Consensus Nomenclature and Process of Care for the Management of Persistent Genital Arousal Disorder/Genito-Pelvic Dysesthesia (PGAD/GPD). J Sex Med. 2021;18(4):665-697. Epub 2021 Feb 19. PMID: 33612417. ↩︎
{kind=link}