

The Serotonin Reuptake Inhibitor (SRI) story starts in 1969 with Arvid Carlsson (above) who created Zelmid, the first SRI, after listening to people on antidepressants. He linked an anxiolytic effect some older drugs have to the serotonin system. The SRIs aimed at exploring that effect – Normality and Antidepressant Dysregulation.
Fluoxetine (Prozac). sertraline (Zoloft). paroxetine (Paxil). citalopram (Celexa). escitalopram (Lexapro), vortioxetine (Brintellix), venlafazine (Efexor) & duloxetine (Cymbalta) are SRIs.
This post aims at giving you a basis for a conversation with your doctor. The so-called patient-information-leaflets (PILs) or even smaller print 40 + pages doctors get are a weapon that is all too often used against you. Give this ‘medicine label’ to your doctor to read, gauge their response and act accordingly – Challenging My Doctor to Disclose.
SRIs
Serotonin Reuptake Inhibitors were created to make you serene – to damp down your reactions – a chill pill. This can be useful for managing stress or anxiety. But no more than half of us who take an SRI become more serene. Some of us become serene but find it unhelpful – just not us. For many of us, nicotine can be better than an SRI.
People who are stressed or ‘depressed’ have normal serotonin systems. If an SRI doesn’t give you a clear and helpful effect within days, you risk a bad trip and should stop. This is particularly true if you feel worse on the treatment.
These drugs are not selective to serotonin. They are not SSRIs. Selective here is a marketing trick designed to fool you. Ditto with SNRIs. These are marketing soundbites not science. SRIs act on multiple systems, producing effects that can add to your stress levels.
The conditions that lead to us being offered an SRI, or told we should have one, on average clear up naturally in 12 to 14 weeks – without treatment. SRIs can help by making things more comfortable while you wait on recovery, but depending on your reaction to different medicines they may be no more helpful for you than nicotine.
SRIs supposedly take up to 6 weeks to work. Stopping treatment earlier, you will hear, would be a mistake. This is a myth. Within days of the first dose, you can notice a numbing of your genitals and emotions – among the good effects – or problem effects like agitation or disinhibition.
Within 2-3 days, people who know you can spot the good and bad changes from the outside, so it is worth letting them know what is going on and paying heed to their input.
If you know you are feeling worse, and your doctor doesn’t listen to you, or suggests this is your depression and needs time or a higher dose, unless s/he is very convincing, you need to change doctor.
Apart from adverse effects, one serious problem is that the help some of us get can mislead us into thinking we would not have recovered without treatment. Even if the drug helps you, your serotonin system will be more abnormal after a few days on an SRI than before and will get more abnormal as time goes on. You will be more resilient if you get well without meds.
Unlike older antidepressants, SRIs can’t help severe depression, melancholia, a condition that affects older people. Melancholia also recovers spontaneously but can take 5-6 months.
SRIs can cause a severe Treatment Resistant Depression (TRD) for which we have no treatments. TRD is not a mood disorder. It is a drug-induced toxic state in which several bodily systems end up badly dysregulated, some of which may never recover.
For some of us, however, SRIs can be more helpful than critics suggest, but neither good nor bad effects are all in our minds – SRIs are no more placebos than LSD is.
Standard SRI doses, the doses most people start on, are close to toxically high. This is because companies had problems showing these drugs worked and couldn’t take a risk on low doses in their clinical trials.
Lower than conventional doses are a safer bet, especially when starting. Fluoxetine 5 mg or perhaps St John’s wort to see if you get the serenic effect and if it suits you. If do not feel anything useful and especially if you feel worse after starting, you should not agree to an increase in dose.
Why keep mentioning nicotine? Arvid Carlsson said for some of us nicotine is better than SRIs. Most of us recognize that nicotine is a poison. If it helps, this is exactly what medicine is about – bringing good out of the use of a poison. We should have the same attitude to SRIs.
You who are taking an SRI are the only person able to decide if the benefits you can detect are worth the risks. SRI risks at the moment look at least as bad as nicotine.
The Drug Label
Company lawyers write Drug Labels/PILs supposedly based on company studies. Regulators like FDA or EMA ‘approve’ what companies write. The regulators do not have the study data. They go along with company efforts to get you on a product that will keep the company healthy, rather than getting you thinking twice about something that may not be right for you.
Companies shape treatment guidelines – standards of care – by ghostwriting the articles on which they are based. The articles often claim a drug worked well and was safe when it didn’t work and was hazardous. Scared of lawsuits, medical journals, guideline makers and lay media won’t hint that a drug might cause problems.
Companies, regulators, medical journals, lay media and increasingly doctors have an allergy to the word cause, unless you are saying a drug caused you to get better.
Companies downplay treatment hazards in ways few doctors know about. The result is a story that puts you at risk from Good Doctors who keep to the Drug Labels and Guidelines written by companies – not by FDA, MHRA, EMA, NICE etc
See Who Will Make Medicine Great Again.
Two mantras help companies eliminate hazards. They claim their randomized controlled trials (RCTs) offer a science of cause and effect. They have branded our views and our doctor’s views as anecdotal. Companies accept RCTs miss some rare or later developing hazards, implying we are told about everything that is common or significant. The best example, perhaps in all of medicine, of how wrong this is lies with SRI induced genital changes that everyone is likely to have within an hour of their first pill. Company trials missed this completely – because investigators were told not to ask about sex.
There is another important feature to RCTs. Even if done by angels, they give average effects. You are not, and no-one is average. You can decide what a drug is doing to or is not doing for you better than anyone else.
Any Magic there might be in Healthcare lies in the relationship between you and your doctor – not in a chemical.
Hazards
SRIs cause the hazards listed here in healthy volunteers. Companies and regulators try to link these hazards to ‘depression’. Mood disorders do not cause these problems.
Sex and Love

SRIs numb genitals and mute orgasms within hours of a first pill, and later diminish libido, in far more people than treatment helps. These problems may recover after stopping but can instead get worse and last decades – this is called post-SSRI sexual dysfunction (PSSD).
SRIs reduce sperm counts in men and hormones critical to embryo implantation in women in addition to causing birth defects. They compromise your fertility. They put any baby you conceive at risk of neurodevelopmental problems. You and your partner should be told this, but we are all kept in the dark and it is no surprise we have falling birth rates.
Emotional Blunting

SRIs aim at making you less reactive. At just the right dose, this can be helpful, but the dose is invariably too high leading to emotional blunting. You may not be able to cry at the funeral of someone you love.
Caring less about consequences may disinhibit some of us. Family and friends may notice personality changes. Other people who have been on these drugs can often spot when you have started an SRI in a way healthcare staff can’t.
See Zen and the Art of Psychopharmacology
Agitation
SRIs can make us malignantly anxious, agitated, irritable or restless and generate out of character thoughts that can usually be distinguished from feelings linked to depression or anxiety. These include impulses to harm ourselves or others, which can lead to suicidal, homicidal, or other criminal behaviour, especially if combined with emotionally blunted disinhibition.
Claims that suicidal effects only happen in young people are incorrect. The treatments can trigger suicidality or homicidality in young or old.
As with sexual effects, family and friends should be made aware of these hazards.
Anyone mentioning anxiety or agitation after starting an SRI may be put on another drug to damp things down or may have their SRI dose doubled. This is dangerous. Stopping treatment should be the first option.
Suicide
SRIs cause suicide, suicidal acts, and suicidal thoughts (suicidality), along with homicide, homicidal, violent or aggressive acts and violent or homicidal thoughts in healthy volunteers or anyone who takes them – whatever age. Forget the idea that it’s your difficult illness that is causing the problems and the answer is to increase the dose. This is possible but less likely than it is the drug causing the problem.
Many of us can distinguish drug induced thoughts like these from anything we might ever have had before. They can begin within hours of a first dose, after a dose change or can be linked to stopping the drug – which can be very tricky.
500 Drugs That Can Cause Suicide
Alcohol

SRIs can increase your alcohol intake whatever its original level was. For some, alcohol damps down the agitation SRIs cause. For others, even pregnant women, drinking becomes compulsive and can cause fetal alcohol syndrome. The combination of an SRI and alcohol increases the risk of other hazards.
Alcohol use often returns to normal almost immediately on stopping the SRI.
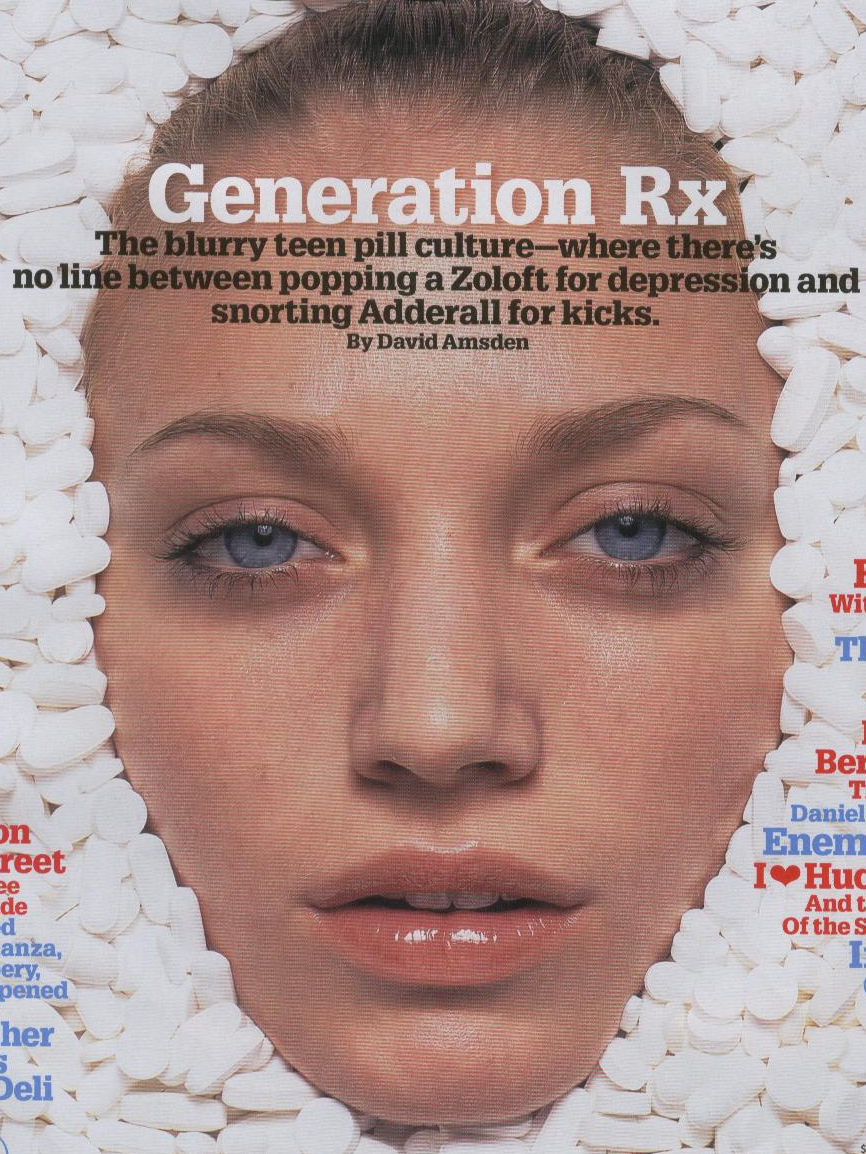
It looks increasing likely that SRIs and other prescription meds may lead to increased intake of non-prescribed drugs. Gen Rx increasingly seem to blur these boundaries.
Conventional drug information tells you nothing about this – Antidepressants and Alcohol
Sensory Problems

Where psychedelic drugs open up the senses, SRIs mute them. Visual Snow is a dramatic visual effect, but SRIs can also cause blurred vision, night blindness, after-images, glaucoma and other problems. Visual Weird Vision Blurred.
SRIs can badly affect balance giving rise not just to dizziness but to a disabling vertigo that leads to a form of panic attacks. None of these conditions show abnormalities on scans and you will be told your problems are all in your mind – and told to take an SRI.
Emotional numbing is closely linked to a literal numbing of touch and other sensations. Too high a dose of treatment or too long on treatment can damage sensory nerve endings and cause pain – for which you will be offered SRIs. This damage is called peripheral neuropathy or sensory neuropathy – as in the image just below.
Dysregulation and Withdrawal

Companies knew from 1980s healthy volunteer studies that SRIs cause serious problems on stopping. Serotonin is more primitive than estrogen and the dysregulation of all our senses SRIs cause trigger a wide range of long-lasting symptoms on stopping equaled only by stopping estrogen in the menopause.
If you have symptoms of anxiety or depression on stopping, your doctor may insist these are part of your depression and you need to go back on treatment or need other meds. This is wrong. Even healthy volunteers get depressed and anxious after 2 weeks exposure, along with nightmares and disturbed sleep.
For some of us, it just takes a few weeks to produce problems stopping an SRI that many people taking opioids find worse that stopping heroin. Stopping can take months or years. Gradual Tapering may help but it may be impossible to stop and take years to get back to normal after stopping.
The withdrawal period has the highest rate of suicidal acts. This leads some to claim SRIs are life-saving. Sexual, vision, balance and other difficulties may get worse in this period. Persistent genital arousal disorder (PGAD) can develop especially in women on stopping and can be bad enough to lead to clitoridectomy.
Acetazolamide or low potency SRIs may make things easier – see RxISK – Antidotes.
Therapists and doctors can make things worse by linking your problems to unresolved trauma. There are an increasing number of people claiming to be able to get you off meds and charging a fortune to do so. No one can reliably get you off at the moment – if you got off without too much trouble you were lucky..
Polypharmacy
SRIs are a gateway drug to benzos, antipsychotics, stimulants, statins, anti-diabetic and other drugs, which may all increase the difficulty in getting drug free and the risk of serious hazards. Company drug labels assume you will only be on one drug. If your doctor has seen fit to put you on an SRI, they are highly likely to want to add other medicines. Every drug they add likely makes the company label for each of these drugs irrelevant.
An SRI in its own right is likely to shorten your life through cardiac or other effects, but a premature death or dementia is even more likely if you are on 3 or more drugs.
SRIs cause muscle wasting as will statins, and weight gain, which along with apathy are liable to make you ever less likely to engage in options that take motivation. Taking a pill will seem easier.
They also seem to be a gateway drug as in the image above to cannabis, adderall etc – Go to the Gym, Eat Vegan and Take Zoloft.
Quality of Life
Back in the 1990s, when SRIs launched, companies, knowing they were less effective than older drugs, pushed a Quality of Life argument instead. Believing their own propaganda, companies made Quality of Life scales and put them into studies,
The data was never published. Why not? You not your doctor complete QoL scales. Those of you on SRIs in company studies reported a poorer quality of life, lower levels of wellbeing, than those not on them.
Other Hazards
RxISK’s Drug Search Tool shows other hazards reported for SRIs. These include weight gain and diabetes, cardiac problems, strokes, bone thinning and fractures, muscle wasting, gut problems, bladder problems, fatigue, sleep problems – on and off the medicines. The list goes on and on. Many of the problems can fool your doctors and you. The urinary tract or prostate infection they think you have may not be an infection and putting you on antibiotics can add to your problems.
You can’t depend on your doctor to get the diagnosis of a side effect right. They are quite likely to put you on other mental health, gut, antibiotic or other drugs for problems that would clear if you stopped your antidepressant.
If a partner or family member is being put on one of these pills you might want to ask them or their doctor to inform your consent. If you are liable to have your love-life wiped out or to be killed or injured by a drug they are put on, should you not be alerted to this? But if you live with someone whose personality changes on a medicine, you might find them resistant to stopping it and their doctor unwilling to listen to you.
Older women used to be the main takers of antidepressants. While there are still many older folk hooked to them, likely forever, older women seem to have gotten the message and are less likely to start them. The number of younger women taking them, however, is rising strikingly. Antidepressants are fast becoming a young woman’s drug.
This is not down to company marketing. These are old drugs from which pharma makes no money now. They also haven’t been shown to work in this age group. What is going on?
We would like to hear from you. Tell us what would make a treatment label work for you and we will write similar labels for other drugs. RxISK wrote Guides to some of these drugs a decade ago and we will update these based on what you tell us you need.
All Illustrations above are by Billiam James
Note:
This post was prepared ahead of a two meetings. First, Washington State’s Congress is exploring consent issues with antidepressants and other drugs in younger people. Britain’s Medicines’ Regulator, also, has been asked to take stock of their risk communications for antidepressants – which at present are very different to those offered here.
Medical Regulatory/Certification Bodies can strike doctors off for using their position as a doctor to promote ‘opinions’ on health matters rather than ‘facts’. Very much aware of this, I am confident this post offers facts rather than opinions.
Finally, this post is the first RxISK post to meet Tik-Tok. There are some great descriptions of the side effects above from Tik-Tokers.
- Lilly describes Emotional and Libido Numbing
- Georgia describes A Bad Trip and is given tricky/scary advice
susanne says
Think you could make it public and patient information leaflet. Forewarned is fore-armed for those caring for any one who needs help with meds
annie says
Judging by Tik-Tok Georgia, she needs to get to the zone; if she suddenly got ‘brain zaps’, her anxiety would do more than ‘go through the roof’. Nobody should be ‘freaking out’
‘Selective here is a marketing trick designed to fool you.’
‘your serotonin system will be more abnormal after a few days on an SRI than before and will get more abnormal as time goes on.’
‘Companies, regulators, medical journals, lay media and increasingly doctors have an allergy to the word cause, unless you are saying a drug caused you to get better.’
THE NEW PIL, FOR EVERY ILL
Tripping the light fantastic
chris says
“Family and friends may notice personality changes. Other people who have been on these drugs can often spot when you have started an SRI in a way healthcare staff can’t.”
This is true. Unfortunately most families and others do not have Tim’s insights, knowledge, intelligence and empathy to correctly engage relatives with severe adverse drug reactions. Jill Nickens and Anne Marie give good insight into all this. Families and others are more likely to be the ones who are on the phone to mental health services demanding their relative be ‘medicated’ because they didn’t smile at the person who served them at the garden centre cafe. They refuse to believe that these drugs that cause severe ADR’s, that are spoken about on here, causing suicide violence to homicide could possible be allowed to go to market. No we are very mentally ill and are in need of constant supervision. Just the other day a relative was boasting about being on their 7th Covid booster and that we need to have the flu jab otherwise we will be terribly ill. It gets alienating, lonely and triesome. We have a target on our faces.
tim says
Amongst so many outstanding and invaluable posts on RxISK and DH Blogs, this is brilliant.
Every detail of this post addresses what is required in terms of information from prescribers (for potential AD recipient patients) that is needed in order for Full, Fair and Informed Consent to be addressed.
In a courageous, dignified and long interview on BBC Radio 4’s Today programme this morning, (07 – 32 GMT) the grieving parents of the late Thomas Kingston provided public health awareness information regarding the risks of SSRIs. It was deeply moving.
They included a recommendation that patients should sign a record of ADR information given to them before an antidepressant prescription is issued.
What would work for me (‘as a treatment label that worked’) would be a coloured,, illustrated patient leaflet given with every dispensed SSRI/SNRI/AD, which contained the information from:
‘Restoring The Magic to Healthcare’ – above.
How many deaths, destroyed lives and heartbroken families could this prevent?
chris says
Thousands and on going.
They should also have interviewed yourself and David to bring precision and expertise to what needs to happen as a matter of emergency as we see horror show after horror show.
To be clear to everyone new to this: It is psychiatric and other drugs which in some people cause them to be suicidal and violent. The condition which causes this is called akathisia, it is almost never correctly diagnosed and is seen as either anxiety or serious mental illness… psychosis depending on how bad the akathisia is. It happens on starting a drug, after sometime being on the drug, if there is a change in dose, going from one drug to another quickly, after the drug has been stopped days, months, even years after.
Harriet Vogt says
There are many disturbing medical facts – as opposed to medicalised ‘truisms’ (Evan Wood’s added value term) – in this post. Even for those of us who are aware of the risks – as well as potential benefits for some – of SRIs.
Definition of TRUISM:
‘Sometimes truisms can be mistaken for factual statements. In fact, despite their seeming obviousness, they are usually opinions.’
https://www.vocabulary.com/dictionary/truism
A fact I wasn’t aware of – but that is ultimately telling – QoL scales – missing in action.
Surely all drugs supposed to ameliorate our states of mind and lighten the burden of the human condition, should deliver a sense of an improved quality of life? How has this omission been skipped over – so lightly?
The other deeply disturbing dimension of this post is the cultural divide between its clinical precision and seriousness – and the way young women seem to be conceptualising SRIs in their conversations on TikTok. How many are paid influencers, who knows? But much of their conversation – comments and answers – seemed to be genuine and experience based.
Not only, as the Generation Rx piece headlined, do they seem to be making no differentiation between Rx and so-called illicit drugs. But ,frankly, I think that’s fair enough – hard to tell the difference these days since, lack of R & D, has meant new drug ideas often seem to be purloined from the illicit sector.
https://adf.org.au/drug-facts/new-psychoactive-substances/
What really bothered me was a tone of voice that was closer to fashion than medicine. The risks of SRIs – particularly a fundamental one – the ‘truism’ that ‘you will feel worse before feeling better’ – was discussed with insouciance – e.g. a peer comment on Georgia’s bad trip ‘Yes, babe been there. It takes 6-8 weeks before it starts to settle.’ When it was perfectly clear that Georgia’s bad trip was very bad indeed – and she needed to get off the drug pronto.
As everyone will know – who read her story and the comments Tiktokers made – Georgia made the smart decision to dump the SRI, despite a lot of advice to tough it out for the karma to come. ‘I stopped taking them as they were doing more harm than good.’ ‘It gets worse before it gets better.’ Yes, I knew this but I just never got better at all, just got worse.’ ‘I come off it in the end and went on ADHD meds once I got my diagnosis.’
‘My diagnosis’ – a badge of honour it seems. Remember the Lexahoe branded sweatshirts.
Stevie says
I never remember having any ill-effects at all starting 75mg Zoloft at 15 and much of my health anxiety and sensory neuroses seemed to disappear, maybe because it ‘muted my senses’. It didn’t seem like placebo, it really seemed to work for me for several years, until it didn’t. It wasn’t until I was briefly tried on Effexor and then put on 10mg Lexapro at 21 that I was diagnosed “Bipolar 2”, tried on Seroquel and eventually Lithium, plus birth control and Accutane for the Lithium acne. I still don’t really understand why the fact that SSRI’s didn’t agree with me didn’t happen for five years.
Twenty years later, after my doctor’s disastrous rapid taper and unsuccessful reinstatement, I developed severe withdrawal and after more than two years I remain incapacitated with balance and vertigo issues and mental and inner akathisia. With regards to ‘muting the senses’, is there anything less toxic and dangerous worth trying? Acetazolamide, Clonidine, Lamictal and Lyrica are the only things I’m entertaining – each with their own risks / issues. Continuing like this indefinitely doesn’t seem feasible.
mary H. says
This is by NO MEANS asking you, Stevie, or anyone else, to rush out and find a prescription for one of the four possible antidotes that you mention but I do have one case to share with you. At our group last night , we heard from a regular participant who has been absent for a while whilst trying to completely withdraw from her prescribed drug. We learnt that she has used Acetazolamide and found that it certainly helped her. She found that it smoothed out some of the difficulties that she was having – such as lack of sleep, which, in turn of course, helped in many ways. After all, a good sleep pattern helps enormously in all manner of ways.
She is completely off her prescribed drug but does not yet call herself a ” success story” – I guess it is early days but, as we reminded her, she HAS successfully withdrawn which was her purpose in looking for something to support her in the first place.
She did say that she had previously tried two different products – neither mentioned in your list – but they failed to support her in any way. In her case it was definitely “third time lucky”.
Please do not just take my word for this as it is a serious decision to make in conjunction with someone who know far more about these things than I do. I just felt that this was worth a mention.
Stevie says
Hi Mary
Thanks so much for chiming in on this. That’s encouraging – may I ask if any of her symptoms involved vestibular issues or akathisia?
It’s great to hear someone had success with Acetazolamide.
annie says
Tune into Marion describing what happened Charlie, her husband, a doctor on an SSRI
https://www.antidepressantrisks.org/stolen-lives/charlie
My name is Marion. I’m a retired psychotherapist and I have been campaigning for the safety of antidepressants.
In 1985 my husband, Charlie, at age 31, was diagnosed with Addison’s disease. He began to recover once started on lifesaving, lifelong medical treatment for this condition. Within a few weeks he had recovered well enough to take up a new position as GP in a small rural practice. He worked full-time as a GP for a further 25 years. In the early 1990’s he was started on Seroxat for depression, commonly experienced alongside Addison’s disease. He remained on 20mg Seroxat until after his retirement in 2010, when he was recommended by a psychiatrist to switch to venlafaxine. This only lasted two months as the side effects were intolerable, and he went back onto Seroxat 20mg which seemed to suit him better. Just a few months later he developed almost complete insomnia, terrors, awful gut issues, severe arthralgia, chronic pain, loss of temperature regulation, paranoia, nightmares, agitation, cognitive issues and altogether felt terribly ill. No-one could seem to fathom what had gone wrong, despite various tests and investigations, adjustments to usual medications and a trial of Melatonin. His notes record an exchange between his GP and endocrinologist where they agree that he is probably ‘somatising’ and ‘just needed stronger antidepressants’. Of course, the Addison’s disease was a significant complication. He was increasingly deeply suicidal and utterly desperate, and acted upon this.
Having now learned of so many unsuspecting souls who have experienced the horrors of medication-induced akathisia, my husband’s ultimately fatal experience following 20 years on Seroxat probably was a form of catastrophic autonomic dysregulation and overwhelmingly intolerable akathisia. He thought he had completely lost his mind.
My hope is that this post will encourage reappraisal and respectful caution about use of these commonly used so called safe and effective anti-depressant drugs, especially when considering starting people on them. Patients and their prescribers need to respect the risks and limitations of these medications so that genuine ‘informed consent’ can be reached before prescribing, or starting to take, any drug. Patients need reassurance that good sense and effective practical and psychological measures can often be taken at the outset to resolve the common symptoms of human stress, emotional turmoil and distress, sometimes without any need for prescribed mental health drugs (including the now emerging trend to develop and market synthetic medical psychedelics), or needing to resort to electrical or other invasive treatments.
annie says
Commending John Montagu, who very recently died, and Luke Montagu, who spoke up
How Antidepressants Ruined Luke’s Life
http://antidepaware.co.uk/how-ads-ruined-lukes-life/
On Dr Collins’s advice, Luke checked himself in to the Priory, where his Clonazepam was withdrawn, although he stayed on Effexor. “I thought I wouldn’t sleep for two or three nights, then I’d be so tired I’d crash out. Instead, it felt like my brain was torn into pieces.”
As Luke was to learn later, Dr Collins had made a dreadful mistake: long-term users of “benzos” need to taper off over months, or even years. Over the next few days, Luke experienced a “tidal wave of horrific symptoms”.
Initially, he couldn’t walk. “I couldn’t co-ordinate my body or judge distances, I didn’t know how far things were away from me. There was this incredibly loud ringing in my ears. I couldn’t see – everything was blurry and I was having flashback after flashback of distant memories, things dredged up from years gone by. I was crying for no reason, sobbing hysterically.
“It was like the detox hell I’d seen in films like Trainspotting. I thought, I’m just going to have to ride this out and it will get better in the same way heroin withdrawal eventually loses its grip. But I had no idea that withdrawal from long-term use of sleeping pills can take months and sometimes years.”
A few days later, Luke discharged himself. “I was in a state of absolute terror. I just wanted to get out of the hospital because I knew that something dreadful had been done to me. Somehow I made it home, but there I realised everything was different. I’d left the house as one person, but returned as another. In a quite literal way, I had lost my mind.”
Since then, Luke has endured seven years of what can only be described as hell. Back home, he found himself unable to focus. “I could barely put a sentence together, remember who I was or what I was supposed to do. It was as if parts of my brain had been erased. For the first couple of years, I had to try to pretend to be the person that I was, while knowing inside that that person had gone.”
Luke continued: “Psychiatry is a corrupt and dishonest business: it treats so-called illnesses that don’t exist with drugs that don’t cure and can cause great harm. And once you have been harmed, it then diagnoses further illness and prescribes yet more drugs.
House of Lords Speaker Addresses Harms From Psychiatric Drugs and Prescription Addictions
https://www.madinamerica.com/2015/06/house-of-lords-speaker-addresses-harms-from-psychiatric-drugs-and-prescription-addictions/
‘
‘the text of a speech by the Earl of Sandwich in the British House of Lords. The Earl criticizes physicians and the government for not recognizing or helping people who are suffering long-term harms from psychiatric medications or who have become unwittingly addicted to certain psychotropics by following their doctors recommendations.’
John Montagu, Earl of Sandwich, dies aged 81
https://www.bbc.co.uk/news/articles/czxke052gdxo
chris says
From the URL bestpsychiatristinlondon
Looks like Luke’s former psychiatrist is still at it:
“patients requiring detoxification from alcohol or drugs who are not ready to commit to a standard 28-day Rehab program”
“standard 28 day Rehab program”
I think Luke settled out of court for a substantial sum – good on him. Wish more were able and in a position to sue their psychiatist and survive it.
annie says
The hardest part, for me, was trying to find a lawyer, in the first place, who was interested.
I rang around many large firms in Glasgow, then tried a smaller firm, who said, he could take on my case, it would cost around 10K, and I wouldn’t win.
Eventually I got hold of someone, in one of the larger firms, by the Clyde, and we met up. She was quite buoyed by my case but said it would all come down to a ‘chosen’ GP, who would be asked about the drug in question, Seroxat. At that point, I knew I was doomed, but persisted anyway.
It took six months for the GP Report to arrive. Her synopsis of Seroxat was more naïve than I expected. Resorting to Wikipedia, and admitting her knowledge of the drug was scanty as in her practice, the drug was hardly used.
The lawyer wrote to me saying she was sure I would be disappointed with the outcome.
In retrospect, if I had to do it again, I would make sure I employed an ‘expert’ for complete back-up to my claims about Seroxat.
chris says
I don’t know how long ago this was, but are you still seriously affected interms of your circumstance or have things improved?
The only thing I’m certain that I stopped is migraine. Five years on and no akathisia so far.. the jury is still out on that. The fear of it returning happens within seconds of waking every day, it gets me out of bed and doing stuff to distract myself.
Reply from NICE
“NICE has not published any guidance on akathisia. I understand this term means restlessness and can be a symptom of another condition or a side effect of some medications. NICE guidance focuses on the management and treatments of conditions or the treatments themselves.”
tim says
Acute, intense AKATHISIA is a life-threatening medical emergency.
Those who have suffered from, or had loved ones lost to AKATHISIA, are rightly concerned about lack of prescriber awareness of this CONDITION, and lack of skill in its MANAGEMENT.
NICE guidance on the management and treatment of this condition, due to Adverse Prescription Drug Reaction (ADR) would surely increase and improve prescriber awareness, diagnosis and management?
‘Restlessness’ is a tragic understatement of the suffering and clinical presentation of this medical emergency. The term ‘Restlessness’ is misleading and predisposes to misdiagnosis.
AKATHISIA GUIDELINE: – Better late than never?
Dr. David Healy says
The problem is not the lack of an Akathisia Guideline or the lack of any decent sense of this and other problems from Drug Labels.
The problem is the lack of a medical description of what people taking these drugs need to know about what can happen as based on medical experience of giving them to people and investigating problems when they happen.
You all should have decent statements for all our drugs – perhaps hosted by BMJ – on the lines of this one here. NICE Guidelines are essentially written by industry. Drug labels are written by industry. Both aim at keeping industry health and covering their back – they are not aimed at informing either any of us who take the drugs or prescribe them.
A NICE Guideline on akathisia is unlikely to be worth the paper its written on
D
chris says
“Friends who knew Harshman also told the outlet that she had struggled with mental health problems, which included post-partum depression. ”
https://www.dailymail.co.uk/news/article-14389481/tranyelle-harshman-shoots-daughters-suicide-fights-life-Wyoming.html
Another horror show I can barely look at save to copy and past the important part with the question was she medicated for this and with what ?
chris says
https://cowboystatedaily.com/2025/02/12/husband-of-woman-in-byron-murder-suicide-says-she-was-depressed-struggling/
“My wife was not a monster,” said Harshman, while weeping.
He began the interview voicing frustration with how quickly news spread of his wife’s suspected murder-suicide before people had the chance to rationalize its possible triggers.
Tranyelle had been dealing with post-traumatic stress disorder, post-partum depression and standard depression, Cliff said.
“Most people don’t understand how that affects the brain. It’s a chemical imbalance,” he said. “And it can be exacerbated by trying to fix it with medication.”
Cliff Harshman declined to go into the specifics of his wife’s treatment, but said she’d been seeking help and receiving treatment.”
susanne says
MP’s tend to fob off anybody who is not one of their own constituents but this could be useful to include in any representations to local MP’s
Bills
Full Debate: Read Full Debate
Department: Leader of the House
Andrew Rosindell
Business of the House
Andrew Rosindell Excerpts
Thursday 6th February 2025
(1 week, 1 day ago)
Commons Chamber
Andrew Rosindell Portrait Andrew Rosindell (Romford) (Con)
– View Speech – Hansard –
–
I would like the Leader of the House to know that a number of my constituents have contacted me regarding the prescribing of antidepressant medicine in the UK and the iatrogenic harm caused to patients by antidepressant medication. Many are now diagnosed and suffering from conditions including post-acute withdrawal syndrome and post-SSRI—selective serotonin reuptake inhibitors—dysfunction. My right hon. Friend the Member for Tatton (Esther McVey) held a Westminster Hall debate on this issue only last year. However, given the severity of the concerns raised, will the Leader of the House consider a full debate in Government time on this very important matter?
Lucy Powell Portrait Lucy Powell
– View Speech – Hansard –
– – Excerpts
I think every MP in the House will have had constituents contact them about the use of anti- depressants, how they are prescribed, their effects, and whether they are fully understood by those they are given to. This is a really important issue, and I will ensure that the hon. Gentleman gets a full response, but I think this would make a very good topic for a debate
mary H. says
Interesting, Susanne, maybe we could add to this level of concern with reports from members of our withdrawal group – could provide a few eye-openers!
susanne says
Go for it Mary!
Parliamentary office
House of Commons
London
SW1A 0AA
Phone: 020 7219 4402
Email: contact@lucypowell.org.
PS Lovely to see the beautiful tapestry again which your group made all those years ago to promote Rxisk
mary H. says
I would love to be able to take praise for the textile piece, as would the rest of our group I’m sure! It is a lovely piece – I actually had Josie create it 3 times in all – each slightly different, of course, due to fabrics used. I still see two of them – my sister was the auction winner and a brother was next highest bidder so he had one and also paid his offer amount into the risk fund. The third was going to be mine but decided to present it as a gift to show gratitude of support received.
I have just sent a link to this week’s post to our MP and also to Lucy Powell and Andrew Rosindell. I doubt if LP and AR will accept the email as we are not constituents but I did head the message as Antidepressant Withdrawal just incase that would make a difference. Shall be looking for more avenues to cover tomorrow!
chris says
https://rxisk.org/restoring-the-magic-to-healthcare/#comment-105196
Tim I referenced you in my reply to them here:
https://rxisk.org/who-will-make-medicine-great-again/#comment-102746
But yes I agree – it wouldn’t be worth the paper it’s written on.
tim says
Seems we both agree on that Chris. I had no wish to be an advocate for guidelines: – Only to increase prescriber awareness of akathisia.
chris says
I apologise for that Tim, was trying to be provocative to NICE not yourself sometimes it’s a real struggle for me to type.
I could not think of anyone better to write the guidance on AKATHISIA for doctors than yourself.