Is the 60-year battle to conquer the Respiratory Syncytial Virus (RSV) in its final phases?
Is bronchiolitis about to be banished for ever? The propaganda might lead you to think so.
Most developed countries from USA to Australia and Luxembourg to Nicaragua have jumped on the bandwagon and give “free” immunisations with either Pfizer’s maternal Abrysvo, given to pregnant mothers, or AstraZeneca-Sanofi’s monoclonal antibody Beyfortus, given to newborn infants. These countries do not need RSV prevention – 97% of infant RSV deaths occur in low-income countries in Africa and India.
Do the benefits of these products outweigh the disadvantages? What do we know about immunity and the response to RSV vaccines?
“Neutralising antibody” (NABs) concentrations can be measured in blood by seeing what concentration of serum neutralises 50% of RSV particles. As different researchers use different tests, measurements may not be directly comparable. But more importantly, how relevant are NABs to immunity?
In healthy adults, RSV NAB levels vary by a factor of 2, probably reflecting the time elapsed since our last RSV infection. Vaccinating not so young adults (over-60) with Abrysvo raises increases NAB levels 15-fold.
According to Astra-Zeneca Sanofi, 25% of newborn babies have no NABs “leaving them particularly Susceptible to RSV infection during their first RSV season.” Happily a shot of Beyfortus on the day they are born can remedy this antibody “deficiency”.
Most babies (75%) have RSV NABs at birth. These naturally occurring NABs fall by 95% during the first year of life during which time all infants get RSV.
The NAB concentrations found in babies born to mothers given Abrysvo while pregnant are 11 times higher than normal. These are pharmacological (abnormal) rather than physiological (normal) levels. Do they give any protection?
The target for both Abrysvo and Beyfortus is the RSV F protein. Antibodies to this protein naturally vary 1000-fold in newborns, which might suggest RSV F is irrelevant.
A Recent Study suggests many infants exposed to RSV during the third trimester of pregnancy are protected but this protection does not stem from NABs.
How much do the RSV antibodies researchers measure have to do with the disease? Is this why 50 years of attempts to find a vaccine for this usually harmless bug have got nowhere?
Good and Bad Antibodies
Most of us know that when we become immune to some infections we also develop antibodies. German Measles is a good example: both the virus and the vaccine can lead to what gets called protective levels of antibodies in blood. But do we hear so much about antibodies because they can be easily measured by regulators and companies?
The Covid pandemic threw up claims that vaccine induced immunity was better than natural immunity and FDA and CDC began approving vaccines, in some cases mandated, on the basis of antibody levels. We may now be seeing an attempt to row back from this – An Evidence-Based Approach to Covid-19 Vaccination.
One of the complications of an antibody approach is that just as the body can make antibodies to a germ, it can make antibodies against a medicine. Antibodies can attack penicillin and cause allergic reactions, which mean you have to avoid the drug completely. This is more difficult when a drug has been shown to be effective and needs to be taken long term or has a long half-life.
Eprex (erythropoetin alfa) is a hormone used to treat anaemic patients suffering from kidney failure. the kidney is the normal source for erythropoietin. Eprex stimulates bone marrow to produce red cells. But Anti-Drug Antibodies (ADA) to Eprex can attack the bone marrow cells making red blood cells and make patients very anaemic.
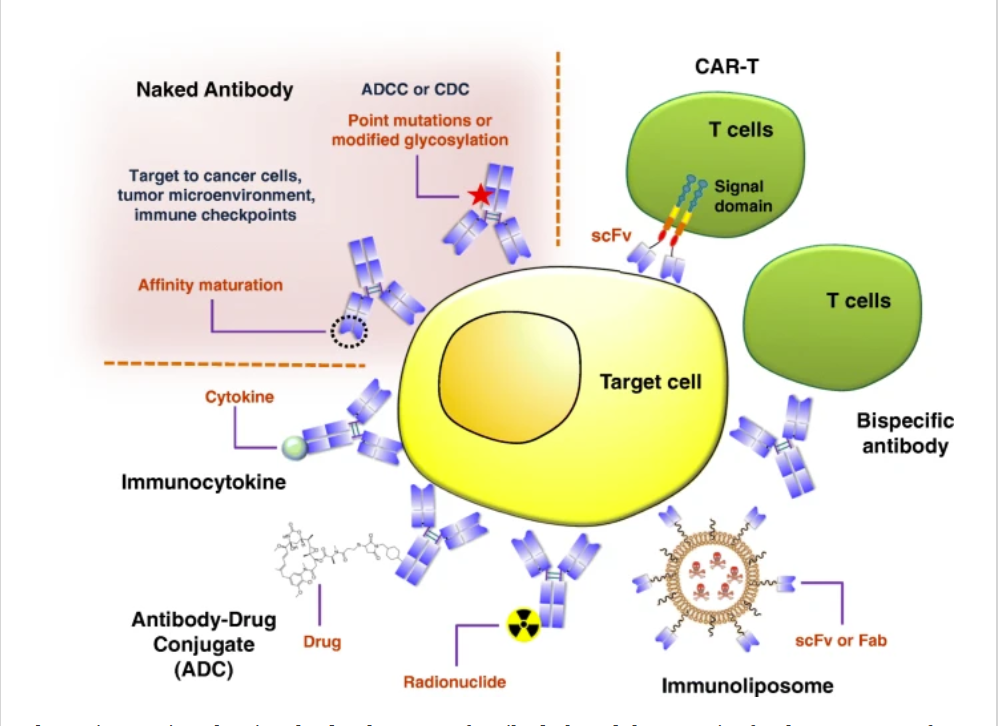
Monoclonal antibodies (MABs) are made in laboratories to attack specific body proteins. They came on stream in the 1990s. They are proteins which means they have to be administered by injection.
MABs like Humira were developed to treat inflammation in Crohn’s disease and rheumatoid arthritis but may also help with multiple sclerosis and now some cancers. Humira became the best-selling drug in the world when its use was extended to minor inflammations like minimal psoriasis. See Letter to Stacey London.
MABs seem particularly prone to triggering ADA, which may seem bizarre. The problem is common enough for FDA in 2019 to draw attention to the risks of developing ADA. What risks? We don’t know.
Theoretically antibodies will stop a MAB from working as well. ADA has been documented for all RSV MABs. Merck have a new RSV MAB Clesrovimab. In trials two-thirds of full-term babies developed ADA to it.
FDA make it clear that no-one knows what else might happen. One of the worries is DRESS – Drug Reaction with Eosinophilia and Systemic Symptoms. This is like a slow motion anaphylactic reaction to Penicillin or peanuts. It can be fatal. See No Way to Treat a Lady. And All Dressed Up Nowhere to Go.
MABs targeted to lower Eosinophil counts are a possible treatment for DRESS, but the same MABs can cause DRESS.
Many psychotropic medications like lamotrigine or antibiotics like minocycline can also cause DRESS and variations on it such as potentially lethal skin conditions like Stevens-Johnson Syndrome or Eosinophilic Esophagitis (our esophagus is continuous with our skin).
RSV MABs
The first MAB to be approved for RSV back in 1998 was palivizumab. This was given to preterm and other at-risk babies. Its disadvantage is that it has to be given by monthly injection. It seemed to prevent RSV in this small proportion of babies but it did not prevent infant deaths or actually treat the disease.
Nirsevimab (Beyfortus) appeared after the patent on palivizumab ran out. One shot is claimed to give a baby six months’ protection. Compared to palivizumab in an RCT of at-risk babies, there were more deaths on nirsevimab.
Despite this, Beyfortus is being rolled out all over the world – except the UK.

Newborn babies under 5 kg routinely have 0.5 ml of liquid containing 50mg of Beyfortus injected into their thigh muscles. One month after the injection average NAB activity is 149 times greater than that at baseline.
These results are from clinical trials in babies averaging 3 months of age. We don’t know what happens to newborns, whose metabolism is different. By comparison a Vitamin K injection routinely given to newborns is a mere 1mg in 0.1 ml of liquid. (A 50 mg dose a large amount for an infant).
By now, almost June, if Abrysvo or Beyfortus given to manage the winter RSV season worked, we should have empty pediatric wards and bored doctors and nurses.
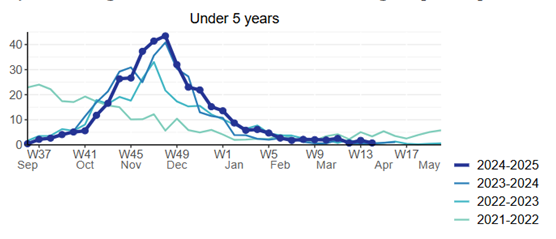
In the UK (Abrysvo territory) children’s hospital admissions due to RSV last winter cannot be said to have fallen when compared to the previous few years (dark blue line below).
In France, where Beyfortus is de rigueur, babies 6-11 months of age, immunised in the previous winter, are more likely to find themselves in intensive care units with bronchiolitis. Black line below (data up to 5 Feb 2025).
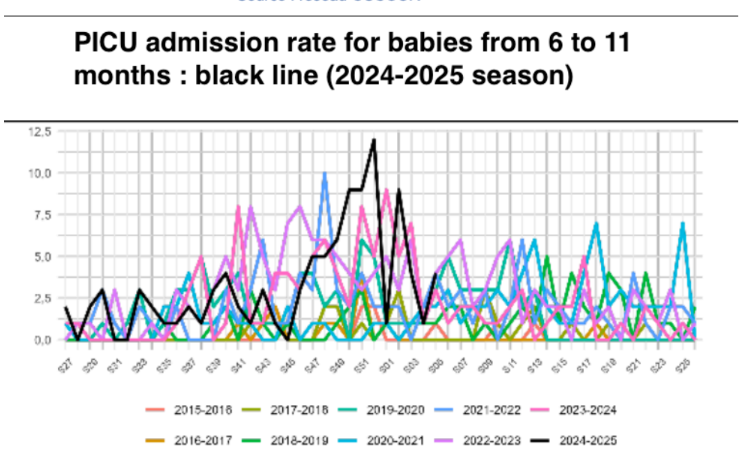
The majority (73%) of under-2s admitted to the intensive care unit with bronchiolitis in France were under 6 months of age, and the bronchiolitis was due to RSV in 62% of cases.
Beyfortus was given to 36% of these cases – leading to claims this shows a reduction of RSV infection admissions. But the increased PICU admissions might stem from more children developing infections caused by other viruses (e.g. hMPV, rhinovirus etc.). RSV, hMPV and other cold viruses are paramyxoviruses. An infection with one confers immunity to the others. Another possibility is that massive antibody levels make false negative RSV results more likely.
Data from Galicia, where neonatal Beyfortus has been the norm for two winters, show that Beyfortified babies who get RSV are as ill as the unimmunised.
In addition to the problems infants have, A Shot in the Dark highlighted the preterm birth risk of maternal vaccination – the suggestion was poohpoohed.
However, a recent BMJ Open review of 6 RCTs and 2 observational studies of maternal RSV vaccination (involving over 20,000 births) confirmed the preterm birth association. The authors used a statistical approach that minimizes the risk but even with this their data point to a real problem.
From Japan, Med Check, edited by Dr Rokuro Hama, has also analysed the Abrysvo data and advises against its use, citing the preterm births, adverse maternal events including preeclampsia, and dubious efficacy in preventing bronchiolitis.
These products look over-rated. What should prospective parents do?
The bottom line seems to be that the safety and efficacy of these products are still uncertain. Beyfortus in particular is breaking new ground being a massive dose of monoclonal antibodies – a class of drug never before injected into the newborn, without any prior safety testing in such young babies.
Breast feeding is effective at reducing RSV disease in children. It also seems likely that the more “colds” due to RSV women have before and during their pregnancies, the better their child will be protected. None of these new products have been shown to save lives.
So why are the relevant paediatric and obstetric professional organisations jumping on the bandwagon of whole-hearted support for these interventions when the grounds for doubts are so strong?
Infallible Papal Immunity
The late Pope Francis was wary about viral respiratory diseases, having had part of his lung removed as a youngster. During the Covid pandemic, he became the first Head of State to mandate the vaccines for all Vatican residents. Three members of the Swiss Guards that protect a Pope resigned

RSV vaccination is being pushed for the not so young. The guidelines recommend Abrysvo up to the age of 80. Francis was 88 but was immunised, perhaps because he was visited by a pal – vaccine enthusiast Fernando Polack.

Frankie didn’t die from an RSV infection, but his doctors kept mentioning a complex respiratory state of affairs. Did Abrysvo make him more prone to hMPV, a rhinovirus or one of the other paramyxoviruses that seem to become more problematic after an RSV vaccine? This was a problem Moderna failed to solve with its mResvia vaccine which combined RSV and hMPV components – see The RSV Virus Challenge.
If Covid or the Flu don’t get you RSV will
The infection probably hasn’t spread to Europe or anywhere else just yet, but it’s pretty virulent in North America, where even the most skeptical and sensible of no-longer young folk (over 60 that is) who have a minor sniffle are now likely to engage with conversations about which of the potentially lethal infections – Covid, the Flu or RSV – they have.
Industry are rushing in to help with self-test kits. The question can be settled.
But be warned, a positive test might lead to social isolation. You are very likely to be banned from seeing your grandchildren. Why didn’t you get the vaccine? That will teach you.

Having a sniffle is harmless. If you have a Covid, Flu or RSV sniffle, the Crucifix and garlic will be held up in front of you – you who have wantonly flouted social norms by not getting the treatment for your vaccine-preventable disorder.
Post by Peter Selley. See Birth Defects Research Vaccines in Pregnancy
annie says
Here is Stat News and Matthew Herper’s take on the Antibody
https://www.statnews.com/2025/05/28/rfk-covid-booster-children-pregnancy-matts-take/
By Matthew Herper May 28, 2025
Robert F. Kennedy Jr.’s unilateral decision that the Centers for Disease Control and Prevention would no longer recommend Covid-19 shots for healthy people during childhood or pregnancy represents a bulldozing of safeguards intended to keep public health officials honest and their decisions transparent. It also tramples on individuals’ ability to make their own decisions about medical evidence.
The decision is deeply and maddeningly ironic, because Kennedy and other top figures in the Department of Health and Human Services are shaped by grievances about how their predecessors behaved during the Covid pandemic. At the time, they railed against decisions that they said were made without medical evidence or the consultation of important experts. Yet Tuesday’s decision to change the CDC vaccine recommendations, as well as new policy made last week about the way Covid shots would be regulated, takes these mistakes and amplifies them.
Instead of slowing medicine’s pendulum so that it might eventually stop at a point of truth, Kennedy, the health secretary, is now swinging it so wildly that patients and doctors can do nothing but cover their heads and duck as medicine becomes more and more vulnerable to politicized extremes.
‘Commissioner Marty Makary and Vinay Prasad, director of the Center for Biologics Evaluation and Research, argued that the U.S. approach to recommending Covid vaccination for everyone ages 6 months and older is out of step with the rest of the world and may no longer be needed’
This seems to be a case of:
‘Having a sniffle is harmless. If you have a Covid, Flu or RSV sniffle, the Crucifix and garlic will be held up in front of you – you who have wantonly flouted social norms by not getting the treatment for your vaccine-preventable disorder. ‘
Dr. David Healy says
One of the points to bear in mind here is that American psychiatry has always been a Swinging Pendulum. Fred Frankel, a psychotherapist given the task of reviewing ECT practices in the US in the 1970s came to the view that
“Something about the American psyche pushed for closure on issues and the sense of certainty that went with closure. There was an intolerance of ambiguity . The only time American psychiatry seemed to be in midpoint was as the pendulum is swinging past it from one side to the other”.
Fred’s observations map back onto a book by Ronald Knox – Enthusiasm. Knox chronicled the history of American Xtian churches – the endless fracturing and appearance of new creeds – the latest enthusiasm. He was warning about the dangers of enthusiasm. But rather than counselling an adoption of cool rationality, he said the most important virtue – the greatest sign of life – is enthusiasm, which back then he figured was more an American thing than a virtue any other nation had.
Have we all become members of the psychiatric domain and not just any psych domain but an American one?
The pendulum can’t swing unless folk like Matthew get worked up about it swinging – is he doing RFKs work for him?
David
annie says
WHO Endorses First-Ever RSV Vaccination Guidance to Protect Infants
https://www.devdiscourse.com/article/health/3442435-who-endorses-first-ever-rsv-vaccination-guidance-to-protect-infants
A Leading Cause of Infant Mortality
RSV is a major cause of acute lower respiratory infections, such as pneumonia and bronchiolitis, in children. Globally, it is responsible for approximately 100,000 deaths and 3.6 million hospitalizations annually among children under five. Infants younger than six months are the most vulnerable, accounting for nearly half of these deaths. Tragically, 97% of RSV-related infant deaths occur in low- and middle-income countries where access to supportive care like oxygen therapy or IV hydration is limited.
Dr. Kate O’Brien, WHO’s Director of Immunization, Vaccines, and Biologicals, emphasized the urgency:
“RSV is an incredibly infectious virus that infects people of all ages, but is especially harmful to infants, particularly those born premature, when they are most vulnerable to severe disease. The WHO-recommended RSV immunization products can transform the fight against severe RSV disease, dramatically reduce hospitalizations and deaths, and ultimately save many infant lives globally.”
Two Immunization Products: A Dual Approach
The WHO position paper offers a dual strategy to address the RSV burden through two promising products:
1. Maternal Vaccine (RSVpreF)
This vaccine is administered to pregnant women during the third trimester (from 28 weeks onwards). The goal is to ensure the transfer of protective antibodies to the unborn child. The vaccine can be given as part of routine antenatal care, ideally during one of WHO’s recommended antenatal visits or additional consultations.
The maternal vaccine, RSVpreF, received WHO prequalification in March 2025, making it eligible for procurement by United Nations agencies and other global partners. The strategy provides passive immunity to newborns, protecting them during their first months of life when they are most at risk.
2. Monoclonal Antibody (Nirsevimab)
Nirsevimab is a long-acting monoclonal antibody given as a single injection to infants. It begins to work within a week and provides protection for at least five months, typically long enough to cover an entire RSV season.
WHO recommends administering nirsevimab:
Immediately after birth or before discharge from a birthing facility,
During the infant’s first postnatal healthcare visit if not given at birth,
Just before RSV season for older infants who have not yet been exposed.
Although the greatest benefit is seen in infants under 6 months, the product can still offer protection for infants up to 12 months of age, especially during their first exposure to RSV.
Implementation Depends on Local Feasibility
WHO’s position paper encourages countries to select the most suitable product based on their healthcare system’s capacity, cost-effectiveness, and population coverage. The Strategic Advisory Group of Experts on Immunization (SAGE) approved both products for global implementation in September 2024. The inclusion of these options is seen as a flexible approach, allowing countries to tailor immunization programs to their public health priorities and resource levels.
RSV: A Common Yet Dangerous Virus
Although RSV typically causes mild symptoms—runny nose, cough, low-grade fever—it can escalate rapidly in infants and other vulnerable groups, leading to life-threatening respiratory illnesses. Premature infants, children with congenital heart or lung conditions, and those with weakened immune systems face particularly high risks of severe complications.
Older adults, especially those with chronic conditions, are also susceptible to RSV, though the new guidance focuses primarily on infant immunization strategies to reduce early-life mortality.
Public Health Impact and Future Directions
The new WHO recommendations are part of a broader strategy to reduce childhood mortality, one of the primary targets of Sustainable Development Goal 3 (SDG3). The implementation of these immunization products can not only alleviate the burden on healthcare systems—by preventing hospitalizations and the need for intensive care—but also ease emotional and financial strain on families.
The position paper aims to guide:
National policymakers setting immunization agendas;
Health program managers integrating RSV strategies into maternal and child health services;
Funding agencies, including international partners and governments, to support the rollout of RSV immunization in high-burden regions.
Looking Ahead
This policy paper is expected to pave the way for broader availability and uptake of RSV immunization products. WHO will continue to provide technical support, monitor real-world impact, and update its guidance as more data becomes available.
The initiative underscores WHO’s commitment to advancing equitable access to life-saving interventions, especially in underserved populations where the stakes are highest.
annie says
‘the Crucifix and garlic will be held up in front of you ‘
Withdrawal of the United States from the WHO — How President Trump Is Weakening Public Health
https://www.nejm.org/doi/full/10.1056/NEJMp2501790
Having worked with WHO country offices, we have seen firsthand how highly valued the agency’s technical guidance is. The guidelines, manuals, and reports it produces are trusted tools for shaping national health policies and improving public health outcomes. The loss of U.S. funding and technical expertise will hinder the WHO’s ability to generate such crucial resources and the capacity of countries relying on them to respond effectively to health crises.
Secretary Kennedy@SecKennedy May 27
I had a wonderful meeting with Argentine President @Jmilei about our nations’ mutual withdrawal from the WHO and the creation of an alternative international health system based on gold-standard science and free from totalitarian impulses, corruption, and political control.
RFK JR: “We’re probably going to stop publishing in the Lancet, New England Journal of Medicine, JAMA and those other journals because they’re all corrupt.”
tim says
Might we have a definition of “Gold Standard Science’?
Dr. David Healy says
There is no such thing as Gold Standard Science. Science involves attempting to arrive at a consensus about things we can observe (see, hear, smell etc) and perhaps work out ways to test whether the consensus is right – what will happen if we vary this or that.
There is no method or machine that delivers understanding. They might help create observables but it is still down to us to reach agreement on what we are seeing happen in a Hadron Particle Collider or an RCT.
D
annie says
RFK Jr. just fired the entire CDC vaccine advisory panel—and it’s just the beginning
As he put it, the real issue is “a history of conflicts of interest, persecution of dissidents, a lack of curiosity, and skewed science that has plagued the vaccine regulatory apparatus for decades.”
Also removed was Dr Eric Rubin, the editor in chief at New England Journal of Medicine. During the pandemic, he defended recommending Covid-19 vaccines for children despite limited safety data.
He stated, “We’re never going to learn about how safe the vaccine is unless we start giving it. And that’s just the way it goes. That’s how we found about rare complications of other vaccines like rotavirus vaccine.”
annie says
Secretary Kennedy@SecKennedy 5h
Yesterday, I retired 17 members of the Advisory Committee on Immunization Practices or ACIP, the @CDCgov external panel that wields the grave responsibility of adding new vaccines to the recommended childhood schedule.
Over the coming days, I will use this platform to announce new members to populate ACIP. None of these individuals will be ideological anti-vaxxers. They will be highly credentialed physicians and scientists who will make extremely consequential public health determinations by applying evidence-based decision-making with objectivity and common sense.
I will also be tweeting examples of the historical corruption at ACIP to help the public understand why this clean sweep was necessary.
The most outrageous example of ACIP’s malevolent malpractice has been its stubborn unwillingness to demand adequate safety trials before recommending new vaccines for our children. Today, a compliant American child receives between 69 and 92 routine vaccines (depending on brand/dictated dosage) from conception to 18 years of age. This is up from 11 shots in 1986. ACIP has recommended each of these additional jabs without requiring placebo-controlled trials for any of them. This means that no one can scientifically ascertain whether these products are averting more problems than they are causing.
Many vaccine promoters have challenged this assertion. They are always wrong.
Last week, @CNN, which has devolved into a shameless propagandist for Big Pharma, triumphantly announced that it had proof that my pronouncement that “there have been no placebo-controlled safety trials for any routine vaccines” was false. CNN gleefully proclaimed that it had found 257 placebo-controlled studies for routine vaccines.
So, allow me a moment to deconstruct CNN’s claims.
Warning: this post may only be sufferable for science geeks like myself.
CNN is wrong. No routine injected vaccine on CDC’s schedule was licensed for children based on a placebo-controlled trial. In instances where a vaccine was used as a control, it too was never licensed based on a placebo-controlled trial. That is not conjecture. It is a fact based on FDA’s clinical trial data. (See http://sirillp.com/noplacebo). As Secretary of @HHSGov, acknowledging this lamentable truth is part of my promise of radical transparency.
The 257 studies cited by CNN unwittingly reflect the lack of safety trials underpinning CDC’s schedule. Despite CNN’s worldwide effort to crowdsource trials with a placebo control (per @US_FDA @CDCgov, an “inert substance”*), this list, on its face, reflects that 236 of the studies clearly did not use an “inert” safety comparator in a trial to license an injected routine vaccine for children on CDC’s schedule.**
For the remaining 21 studies CNN’s list claims used an inert injection, 9 plainly did not:
• RCT 251, 252 (Varivax) injected an antibiotic, neomycin – not inert.
• RCT 84, 97 (HPV-16 and 16/18) injected aluminum adjuvant – not inert.
• RCT 215 (Almevax) injected another vaccine – not inert.
• RCT 55 (Lyophilized PedvaxHIB) injected lactose, aluminum adjuvant, and thimerosal – not inert. • RCT 197 (Salk vaccine) injected 199 solution, synthetic tissue culture, ethanol, phenol red, antibiotics, and formalin – not inert.***
• RCT 168 (Dow’s MMR) injected full vaccine minus virus, including all stabilizers, antibiotics, diluent, preservative, and buffers – not inert. ****
• RCT 189 (Menveo) injected Tdap+saline or Menveo+saline – not inert.
For the remaining 12 listed studies which may have had an inert injection, none was a trial relied upon to license a routine vaccine on CDC’s childhood schedule:
• RCT 170, 171, 172 (MMR VaxPro), 228 (PCV11), 136 (Vaxigrip), 242 (Antitetanus), and 122 (Chinese flu shots) trialed vaccines never licensed in the U.S. nor relied upon to license a U.S. vaccine.
• RCT 124 (Fluzone IIV3), 102 (WVV/SPV), and 188 (Menveo) trials occurred after each respective vaccine was licensed, hence were not relied upon for their licensure. • RCT 176 (Mumps vaccine) was not relied upon by the FDA to license the current MMR vaccine. (See MMR-II clinical trial report in link above.)
• RCT 53 (PRP-D) was for a vaccine withdrawn soon after its introduction and not relied upon by the FDA to license any U.S. vaccine.
While these 12 studies were not relied upon to license a routine vaccine on the CDC’s schedule, they do reflect that a placebo-controlled trial of a vaccine is possible. They also reflect what can be learned when a placebo trial is performed. For example: RCT 136 found the vaccine ineffective; RCT 122 found that “severe adverse effects occurred in 69 (0·6%, 95% CI 0·5–0·8) recipients of vaccine compared with one recipient (0·1%, 0–0·2) of placebo.”; and RCT 124 found “the rate of hospitalization was actually higher in the [Fluzone IIV3] vaccine group than in the placebo group.”
The unfortunate reality is that placebo-controlled trials, however, do not occur and have not been relied upon when FDA licenses vaccines for injection during childhood or ACIP recommends the shot for addition to the CDC’s routine schedule.
CNN would have reached the same conclusion had it reviewed the FDA documentation for each vaccine, instead of relying upon a random, crowd-sourced list from the internet. CNN’s list ironically proves the lack of adequate safety trials for routine childhood vaccines.
It is time to stop playing games, such as CNN’s false gotcha. We have gone from 3 routine injections by age one in 1986 (the year the National Childhood Vaccine Injury Act passed) to 25 routine injections by age one in 2025 (which now does not include Covid-19 vaccine). Because of the 1986 Act, every one of these products, save one, was developed by companies knowing they would almost never be liable for serious harm. During this same period, chronic diseases in our children exploded, most of which are caused by immune system dysregulation. If we are to identify the exposures that are causing this epidemic of autoimmune diseases, we need to rule out products given dozens of times to young children, specifically to modify the immune system, as potential culprits.
Our infants and children deserve the best safety trials possible to keep them safe. We should care as much about every child who could be injured by one of these products as we do every child who could be injured by an infectious disease. We must protect all children.
Notes:
* https://fda.gov/media/130326/download… (“Placebos, defined as inert substances with no pharmacologic activity, are commonly used in double-blind, randomized controlled clinical trials.”); https://fda.gov/media/71349/download… (“the placebo control design, by … including a group that receives an inert treatment…”); https://cdc.gov/vaccines/glossary/… (“Placebo: A substance or treatment that has no effect on living beings, usually used as a comparison to vaccine or medicine in clinical trials.”). **
While the above addresses injected vaccines, CNN’s cited list also includes 10 trials for rotavirus vaccine, given by oral drops, but none of these trials used saline only drops. Instead, RCT 205, 207, 208, 209, 210, 213 (Rotarix) contained dextran, sorbitol, amino acids, dulbecco’s modified eagle medium, calcium carbonate, and xanthan; RCT 211, 212 (RotaTeq) contained polysorbate 80, sucrose, citrate and phosphate; and RCT 206, 214 (Rotavac) included neomycin sulphate, kanamycin acid sulphate, trehalose, lactalbumin hydrolysate, human albumin, potassium dihydrogen orthophosphate, dipotassium hydrogen orthophosphate, and trisodium citrate dihydrate. The list also included three trials of an inhaled flu vaccine; the controls in RCT 104 were OPV+saline or LAIV (a vaccine), hence neither inert; in RCT 106 the control “consisted of normal allantoic fluid harvested from uninfected eggs stabilized with sucrose–phosphate–glutamate”; and, in RCT 109, the control was “intranasal spray of egg allantoic fluid containing sucrose-phosphate-glutamate.” ***
Note that the current polio vaccines used in the U.S. are a different product than the polio vaccine developed by Jonas Salk in the 1950s—which was discontinued in the 1960s—including because the currently-used polio vaccines are “grown in vero cells, a continuous line of monkey kidney cells cultivated on microcarriers.”
Hence, the Salk trial was not relied upon to license any current polio vaccine.
https://fda.gov/media/75695/download…; https://pubmed.ncbi.nlm.nih.gov/6740101/;
https://http://admin.phe-culturecollections.org.ukmedia/122249/vero-cell-line-profile.pdf;
https://atcc.org/products/all/ccl-81.aspx#characteristics….
**** Dow Chemical’s MMR vaccine used different strains than any licensed U.S. MMR vaccine and also, after 14 days of safety review, this trial vaccinated all participants.
https://www.bbc.co.uk/news/articles/clyge27y2g9o
Acip has a meeting scheduled starting 25 June, at which members are scheduled to vote on recommendations for vaccines for Covid, flu, meningococcal disease, RSV and other illnesses.
Dr Brewer said Acip had some of the “best scientists in the world”, adding that the secretary would have a hard time finding that calibre of experts again on short-term notice.
https://edition.cnn.com/2025/06/09/health/rfk-cdc-vaccine-advisers-removed
“This decision will make it far more difficult for pediatricians and other providers to care for their patients. The idea that ACIP has failed to scrutinize vaccines being given to pregnant women and babies is absolutely absurd,” Besser said.
Peter Selley says
Kennedy calls the shots and names new ACIP members
https://edition.cnn.com/2025/06/11/health/kennedy-new-members-vaccine-advisory-panel
Dr. Robert Malone – a physician and vaccine critic who conducted early research on mRNA vaccine technology.
Dr. Joseph Hibbeln – a psychiatrist and neuroscientist who was formerly the acting chief of the section of nutritional neurosciences in the Laboratory of Membrane Biophysics & Biochemistry at the National Institutes of Health.
Dr. Martin Kulldorff – a biostatistician and epidemiologist, who was dismissed by Mass General Brigham last year and, as a result, fired from his faculty position at Harvard Medical School. He had slammed the university for how it handled the Covid-19 pandemic. He has served on the Food and Drug Administration’s Drug Safety and Risk Management Advisory Committee and the CDC’s vaccine safety subgroup of ACIP.
Retsef Levi – a professor of operations management at the MIT Sloan School of Management who has also served as faculty director of the school’s food supply chain analytics and sensing initiative.
Dr. Cody Meissner – a professor of pediatrics at the Geisel School of Medicine at Dartmouth. He has held advisory roles with both the CDC and FDA, and has been a voting member of ACIP and the FDA’s vaccine advisory committee
.
Dr. James Pagano – a board-certified emergency medicine physician who has served on multiple hospital committees.
Dr. Michael Ross – a clinical professor of obstetrics and gynecology at George Washington University and Virginia Commonwealth University. He has served on the CDC’s Advisory Committee for the Prevention of Breast and Cervical Cancer.
Vicky Pebsworth – a nurse with a PhD in public health, who has previously served on FDA vaccine advisory committees.
annie says
A closer look at the new members of the CDC vaccine advisory panel
Several of those picked by RFK Jr. have a history of vaccine skepticism
https://www.statnews.com/2025/06/11/rfk-jr-vaccine-advisory-panel-new-acip-members-include-mrna-skeptics-covid-critics/
I am quite sure the complete article will be less than complimentary about RFK Jr. picks for the new members of the CDC vaccine advisory panel. STAT authors are missing the point that the whole point is to study why ‘vaccine skeptism’ exists.
Children’s Health Defense@ChildrensHD Jun 11
FDA Greenlights Merck’s RSV Shot for Newborns — Clinical Trials Showed 11.71% Rate of Serious Adverse Events, Including Death
The clinical trial results posted on the government website http://ClinicalTrials.gov included serious neurological adverse reactions that Dr. Peter Selley, a U.K. general practitioner who has closely followed the development of the drugs for RSV, called “concerning.”
These included febrile convulsions, seizures, facial paralysis and brain injury at about three times the rate in the vaccine group (25 of 2,409) as the placebo group (4 of 1,202).
Children’s Health Defense Senior Research Scientist Karl Jablonowski said the trials showed a serious adverse event rate of 11.71% and included:
A 50% greater chance of death (three deaths in the group that received the shot versus one in the placebo group). A 350% greater chance of an upper respiratory tract infection. A 63% greater chance of a lower respiratory tract infection. A 41% greater chance of febrile convulsion.
Read more from Brenda Baletti, Ph.D. on CHD’s The Defender
https://childrenshealthdefense.org/defender/fda-merck-rsv-shot-newborns-clinical-trials-showed-serious-adverse-events-death/
However, Selley cautioned that “more is not better.” He told The Defender:
“The implications of this are that with only one dose of clesrovimab, tiny preterm babies under 5 kilograms are going to be injected with a relatively much bigger dose of the monoclonal antibody, leading to massive levels of the drug in their circulation.
“In most other fields of medicine, the aim is to find the lowest dose of a drug that is effective, as most side effects are dose-related.”
The CDC vaccine advisory committee, which makes vaccine recommendations, is scheduled to meet June 25-27 to make recommendations for Enflonsia and several other shots.
However, following Monday’s announcement by U.S. Health and Human Services Secretary Robert F. Kennedy Jr. that 17 committee members will be retired, effective immediately, it’s unknown if the new committee will recommend the shot this month.
Dr. David Healy says
Alain Braillon recently offered a comment in another forum that seems pertinent here:
Anselem and colleagues must be commended for their study about influenza vaccination during pregnancy in France in 2021 showing that vaccination was only “offered” to 59% of women, 54% of them being not vaccinated [1]. However, their ”identification of the key points” to improve uptake of “despite a French national recommendations since 2012” deserved questions.
Could the issue be the French High Council for Health’s 2012 recommendation that all pregnant women must be vaccinated against influenza [ref. 17 in 1]? Indeed, it failed to rate the level of evidence and to document benefits on relevant clinical outcomes. Furthermore, neither tools for targeting professionals and women for implementation, nor funding for quality assurance to monitor it. Prevention is about a public health program by professionals who must be accountable for results not incantatory hypes to please a Department of Health.
Why did the Council fail to provide adequate information and to update its recommendation? The pillars of shared decision-making are: a) common-sense pictographs that use absolute numbers with a consistent denominator, time frames and visuals employing the same scale for information on gains and losses of the options; b) accepting the person’s decision based on his values [2]. I was unable to find on the Internet a publication with the Number Needed to Vaccinate (NNV) to prevent a relevant clinical outcome. Are vague claims of effectiveness, avoiding absolute numbers, from trials in developing countries relevant [ref. 10-13 in 1]? There is only one reliable observational study in a developed country, it reported relative risk reductions [3]. The calculation of the number of pregnant women to vaccine to prevent one influenza-associated hospitalization in infants gives 67. It may vary on factors like the influenza season, vaccine effectiveness, and regional infection rates. Of note, the median duration of hospitalization was one day and there was no effect on ICU hospitalization, NNV being 35,759. Last, a healthy bias may have favored benefits as non-vaccinated women were more frequently non-Hispanic Black, publicly insured, not breastfeeding [3].
Last, how can the Council ignore that silo strategies are rarely effective? Regarding vaccination the issue is also about other respiratory viruses (syncytial, whooping cough, not to account COVID-19). Furthermore, according to the NHS, vaccinations only rank 7th among things pregnant women can do to keep them and their baby as healthy as possible; they begin with not smoking, not drinking alcohol and folate supplementation [4]. Of note, France has one of the highest stillbirth rate in Europe and in 2021, 12% of women reported smoking during the third trimester of pregnancy [5].
I’m afraid that the Council’s recommendation for “influenza vaccination during pregnancy and obesity” [ref. 17 in 1] is a programed failure, on the form as on the substance. Regarding the latter, disinformation (that is not only false or misleading data shared unintentionally but also poor quality data) is a gateway for disinformation (deliberately deceptive information) by anti-vaccine advocates.
References
[1] Anselem O, Charlier C, Viaud M, Lelong N, Vaux S, Launay O, et al. Barriers to influenza vaccination during pregnancy in France: A national population-based study. Vaccine. Published online January 3, 2025. doi:10.1016/j.vaccine.2024.126671
[2] Braillon A, Bewley S. Shared Decision-Making for Cancer Screening: Visual Tools and a 4-Step Method. JAMA Intern Med. 2015;175(11):1862. doi:10.1001/jamainternmed.2015.4721
[3] Sahni LC, Olson SM, Halasa NB, Stewart LS, Michaels MG, Williams JV, et al. Maternal vaccine effectiveness against Influenza-associated hospitalizations and emergency department visits in infants. JAMA Pediatr 2024;178(2):176–84.
[4] National Health Service. Your NHS pregnancy journey. 1 August 2022. Available at https://www.nhs.uk/pregnancy/finding-out/your-nhs-pregnancy-journey/
[5] Peyronnet V, Le Faou AL, Berlin I. Sevrage tabagique au cours de la grossesse [Smoking cessation during pregnancy]. Rev Mal Respir. 2024;41(9):685-695.
Peter Selley says
A Dressing Down
The US equivalent of the UK Yellow Card Scheme’s attempt at pharmacovigilance is FAERS (1). Here there is a mountain of data stashed away – with the proviso that reporting of adverse drug events is highly selective and does not prove cause and effect.
It is interesting that a team from Peking thought it important to examine reports of DRESS to FAERS (2). In the 20 years up to 2023, 0.13% of adverse events submitted to FAERS (15,751 of 11,737,133) was identified as DRESS. There were 1,043 fatal cases, although of course DRESS is often undiagnosed.
What they found was that the top culprit associated with DRESS was allopurinol, frequently prescribed to prevent gout.
And allopurinol was the drug most associated with fatal outcomes. Deaths were reported almost 3 times as often in those with DRESS associated with allopurinol than in those whose reaction was linked to lamotrigine. Perhaps warnings of dangerous skin reactions are more likely to be given when the newer drug, lamotrigine is prescribed.
In the UK in the same period there were 23 “skin” reactions reported linked to lamotrigine (3), with 2 deaths, and 43 reactions including 13 deaths associated with allopurinol (4).
Unlike for lamotrigine, in the UK the allopurinol patient information leaflet contains no warning of DRESS as a potential serious adverse reaction, yet allopurinol is prescribed much more frequently.
1 https://www.fda.gov/drugs/fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard
2 https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2024.1490334/full
3 https://yellowcard.mhra.gov.uk/idaps/LAMOTRIGINE
4 https://yellowcard.mhra.gov.uk/idaps/ALLOPURINOL
Dr. David Healy says
Peter
This is tricky. There are over 6000 deaths when checking OpenFDA/FAERS through RxISK’s Drug Search tool. And there are more reactions linked to lamotrigine than allopurinol. Part of the problem is that some reports are for Lamictal and slightly less for Lamotrigine – but added together more than for allopurinol.
There are more reports for carbamazepine than allopurinol – and add Tegretol in and it becomes far more reports. Generally anti-convulsants seem to be the drugs most likely to cause this problem – by a long way. And of course pretty well all anticonvulsants cause fetal valproate type pictures – autism spectrum disorders.
Pursuing that path further, acetaminophen (paracetamol – Tylenol) also causes DRESS very commonly and is an anticonvulsant. Which for me raised the question – is allopurinol by any chance an anticonvulsant and it appears that it is. It has been pigeon-holed as a gout treatment but is also used an an adjunctive anticonvulsant and for refractory epilpsy.
Who knew? I’ve no idea why you chased this allopurinol lead – what led to it – please tell us – but it seems a fertile one.
David
Dr. David Healy says
Response from Peter
The Chinese looked at it the other way – searching for DRESS, finding 15,751 in 2003-2023 and then looking at the suspect drug and the 1,043 deaths in notified DRESS Do you think their data is wrong?
Why I put this up was because I used quite a bit of allopurinol and was unaware about DRESS risk or deaths.
Dr. David Healy says
Peter
There are definitely issues to chase. Putting Drug Rash with Eosinophilia and Systemic Symptoms into RxISK’ side effect search gives 11000 + – less than the Chinese 15,000+. But entering Drug Reaction with Eosinophilia and Systemic Symptoms in RxISK gives 74,000+.
This is surprising because if you change the entry and put Eosinophils rather than Eosinophilia – you get 0. The system usually wants you to be precise but it looks like it might tolerate some surprising differences for this problem.
The 6000 deaths was for allopurinol – not DRESS deaths. Overall there are 500,000 + adverse effects compared to 780,000 + on sertraline – so comparatively that’s a lot of problems on allopurinol.
Looking at the DRESS reactions they are what you’d expect – anticonvulsants, antibiotics, MABs and SSRIs.
The RxISK Drug Search and Side Effect Search tools throw up some fascinating leads
David
Dr. David Healy says
I meant to add one more comment. Way back when Prozac had a lot (20+) solid article proving it caused suicide – these had very little impact. The company – its the disease – argument worked well.
At the same time, there were very few reports of convulsions on bupropion – which was heavily restricted, used minimally companed with company hopes and never licensed as an antidepressant in the UK.
Is DRESS a hide-able problem? With some vaccine reactions etc it can almost certainly be buried as part of the Covid we were trying to avoid. Antibiotics? Maybe similar. It may be prominent in Gout because it’s hard to palm off as not linked to the med rather than the illness.
The drugs that cause it seem generally risky in pregnancy
D
Peter Selley says
Another problem is that there is an “Allopurinol hypersensitivity syndrome” which overlaps with DRESS.
https://en.wikipedia.org/wiki/Allopurinol_hypersensitivity_syndrome
Does the Rxisk drug search rely on OpenVigil which is what the Chinese team used to interrogate FAERS?
Dr. David Healy says
Allopurinol hypersensitive syndrome does not feature in pharmacovigilance databases per se – its not MedDRA coded. Open Vigil accessing FAERS is roughly similar to RxISK accessing Open FDA. There may be minor differences but little that is consequential.
The most consequential likely to be the RxISK data has two more years worth of data than the Chinese paper had access to
D
Harriet Vogt says
I’ve been looking into these RSV vaccines, not with your/ Peter’s scientific eye, but as a consumer of public healthcare information.
It’s perfectly clear from reading between the lines of the NHS statements that, as Peter says, there is actually no need for the maternal vaccination:
‘Most cases can be managed at home but around 20,000 infants are admitted to hospital with bronchiolitis each year in England. Infants with severe bronchiolitis may need intensive care and the infection can be fatal. RSV is more likely to be serious in very young babies, those born prematurely, and those with conditions that affect their heart, breathing or immune system.’
https://www.gov.uk/government/publications/respiratory-syncytial-virus-rsv-maternal-vaccination/a-guide-to-rsv-vaccination-for-pregnant-women
The 20-30 little souls who die each year in the UK are the extremely vulnerable to start with – including those born prematurely (alarm bell tinkling).
The healthcare business objective is clearly to save time and money on hospital admissions. The first year figures Peter shows, suggest they’re not much cop at that. But the caveat is only a 30ish% uptake of the maternal vaccine, and the figures aren’t broken out by vaccinated and unvaccinated mothers anywhere, are they? There’s of course a new condition that has entered the marketing health lexicon – ‘vaccine hesitancy’ – a distant relative of ‘treatment resistant depression’ . (polydrug toxicity to anyone who learned not to mix their drinks).
What really concerns me is the cavalier way in which the clear safety signal for preterm births –is dismissed in the UK:
‘The safety of RSV vaccination during pregnancy
The vaccine has been studied in clinical trials of almost 4,000 women and been given to many thousands of women in national programmes.
Monitoring in the USA, where it has been given to over 300,000 women, has shown a good safety profile. In the main clinical trial, in the month after vaccination, there were slightly more premature babies in the vaccine group (2.1%) than the group that didn’t have the vaccine (1.9%). This difference is most likely to be due to chance.’
Statistics are a theoretical way of seeing (miraculously ,I passed a stats module)- but the commonsense way says, pay attention, something is happening here. I hope the rate of preterm births is also being tracked – can’t find it.
It seems perverse that even the FDA regards the safety signal as sufficiently indicative to recommend vaccination between 32-36 weeks, But here in the UK, the powers that be are happy with 28 weeks when – so AI tells me – there is an 80-90 survival rate ,with a 1 in 10 chance of long term health problems , whereas by 32 weeks the survival rate is 99% and nigh on 100% between 32-36 weeks.
And guess what, as far as I can see, this risk isn’t even mentioned in the PIL – surely it should be?
https://www.medicines.org.uk/emc/files/pil.15309.pdf
I had a quick look at a manufacturer funded ‘pragmatic trial’ of the infant vaccination, nirsevimab, published in the NEJMisinfo, that had received a fair bit of press coverage. Playing the usual, ethically unacceptable reporting tricks – percentages rather than actual numbers:
‘The efficacy of nirsevimab against hospitalization for RSV-associated lower respiratory tract infection was 89.6% (adjusted 95% CI, 58.8 to 98.7; multiplicity-adjusted P<0.001) in France, 74.2% (adjusted 95% CI, 27.9 to 92.5; multiplicity-adjusted P=0.006) in Germany, and 83.4% (adjusted 95% CI, 34.3 to 97.6; multiplicity-adjusted P=0.003) in the United Kingdom.
But the adverse effects were swiftly swept under the carpet:
‘Treatment-related adverse events occurred in 86 infants (2.1%) in the nirsevimab group’.
In fact, there were 1479 adverse effects for babies on the drug vs 1326 on standard care – 89 of which were classed as serious vs 67 in the standard care group. https://www.nejm.org/doi/full/10.1056/NEJMoa2309189#t2
Ultimately what I find particularly unsatisfactory about all this – apart from the dodgy ‘science’ and unnecessary risks – is that, as Peter mentions, breastfeeding is a natural, on tap source of antibodies and healthy infant nutrition. And not just that – as we know, it has a protective effects against breast cancer, helps us women recover our pre-pregnancy bodies – and our offspring are less likely to be overweight in the future.
https://www.breastcanceruk.org.uk/breastfeeding-and-breast-cancer/
It’s a shocker that the UK is one of the countries in the world least likely to breastfeed for the recommended 6 months. Of course, there are loads of obstacles – especially the need to return to earning to survive.
But you’d think – I would anyway – that any government with an holistic view of public health would do its best to create conditions that give mothers every opportunity to breastfeed. But, no, they’d rather dish out jabs and fail to control the sales’ messages of formula manufacturers. And of course there’s always semaglutide to help the overweight adult babies –notwithstanding risks to the digestive system, kidneys etc.
It is dystopian that medicalisation has reduced whole human beings to dislocated bits of disparate biological and psychological function.
Peter Selley says
Harriet
I wish there were more “lay” views because most “scientists” can’t see the wood for the trees.
Pfizer’s Abrysvo study reported “any cause” lower respiratory infections (i.e due to RSV and all the other viruses combined) needing medical attention. The results showed that the vaccine was only between 2.5% and 7.0% effective. (Table S8)
https://www.nejm.org/doi/suppl/10.1056/NEJMoa2216480/suppl_file/nejmoa2216480_appendix.pdf
80+% efficacy in babies in almost all the headlines is specific to RSV disease in the RSV season, rather than ALL chest infections, of ALL causes, in the year or two following immunisation.
These data – from the original pivotal study – showed that the vaccine would not lead to fewer infant medical consultations and financial savings.
When Pfizer was confronted by the FDA over the preterm babies concern they hatched a deal to organise postmarketing safety surveillance. Too little too late.
The agreed projects are listed here
https://www.ema.europa.eu/en/medicines/human/EPAR/abrysvo#related-medicines
For instance The BERNI trial is being run in Argentina and Uruguay by Pfizer-friendly Fernando Polack’s i-TRIALS (q.v.) and aims to report by January 2027. The results, when they eventually come, wont be much help in the UK where women are vaccinated at 28 weeks, rather than at 32-36 weeks of pregnancy in those countries.
The FDA and Pharma are laughing all the way to the bank.
For more about these deals, see the recent self-explanatory https://www.levernews.com/fda-approved-and-ineffective/
Dr. David Healy says
Pharma laughing all the way to the bank sounds right. Would FDA be laughing?
Joe Toerner, the FDA guy juggling with all this, has left the agency – perhaps now with pharma – but clearly figured that medicine rather than FDA had a role to play in calling the shots. Doctors aren’t laughing all the way to the bank. Junior doctors in the US are increasingly unionising because of pressure from the companies they are now employed by to stick to what is legally defensible – as all good employees should – what is good for the health service company they work for rather than what is good for their patient.
Doctors should be standing up but aren’t. It’s not FDA’s job to stand up – other than to get the wording of the labelling right as Joe Toerner ex-FDA told us – see the December 2023 Uterine Roulette and Consent RxISK post. The wording in the US FDA agreed to was almost certainly crafted by Pfizer.
D
Harriet Vogt says
Peter
I do also somertimes feel that the ‘scientists’ have lost their common senses
– and actually wonder if all the convoluted ‘scientism’ around these drugs – is deliberate marketing obfuscation.
I’ve been having another ‘lay ‘ rummage about in the public information. As you have always said, there is clear evidence – even of a ‘statistically significant’ variety– that preterm births are a real risk.
‘Results VAERS received 77 reports pertaining to RSVpreF vaccination in pregnant individuals, with 42 (54.55%) classified as serious. The most frequently reported non-pregnancy-specific AEs were headache, injection site erythema and injection site pain. For pregnancy-specific AEs, preterm birth was the most frequently reported (12.8%), followed by AE terms such as preterm premature rupture of membranes and caesarean section (each at 3.3%), and cervical dilatation, haemorrhage during pregnancy and uterine contractions during pregnancy (each at 1.4%). Our disproportionality analysis indicated signals for various AEs, particularly preterm birth, indicating that reports of preterm birth in conjunction with RSVpreF vaccination were observed more frequently than statistically expected. Most of the reported preterm births were moderate to late, occurring between 32 and less than 37 weeks of gestation. The median time from immunisation to the onset of preterm birth was 3 days, with two-thirds of cases reported within a week of vaccination’.
https://bmjopen.bmj.com/content/15/4/e087850
Hence the absence of any mention from the UK PIL is surely negligent?
I’ve also discovered that, despite one assumes being aware of this risk of preterm birth, the EMA has granted market authorisation from 24 weeks! AI would suggest that this is dangerously irresponsible.
‘Survival Rates:
While survival rates vary, many resources estimate that babies born at 24 weeks have a survival rate between 42% and 68% according to ACOG and some studies.
Long-term health problems:
Babies born prematurely at 24 weeks are at risk of developing long-term health issues, including cerebral palsy and blindness.’
I’ve just tripped over a company driven safety study protocol, winningly branded – PROMISE – preparing for RSV immunication (this is a typo – rather apt – so I let it stand) and surveillance in Europe. The promise is to assess safety by comparing matched samples of pregnant women 24-36 weeks gestation, vaccinated vs not.
https://usher.ed.ac.uk/sites/default/files/atoms/files/promise_d2.9_generic_protocols_safety_in_pregnancy_and_older_adults_v1.0.pdf
I’ve just managed to glance at the front page of the Sunday Times, today:
‘Children’s jabs for deadly disease slumps to lowest level in a decade’.
And there we have it – the adverse effects of the great vaccine sale bonanza on public health.
‘Anti-vaccine sentiment is on the rise… YouGov found the percentage of people agreeing that vaccines causing harmful effects that were withheld from them had risen from 14% (during Covid vaccine rollout to 34% this year’.
If the system keep lying about vaccine and drug safety – patients and families will cease being able to see the wood from the trees too.
Peter Selley says
The only way is up, baby
How low are doctors prepared to stoop?
According to its manufacturer, Merck, clesrovimab’s main advantage is that it has the potential to become the first and only approved immunization designed to protect infants with the same single dose regardless of weight.
Clesrovimab is merely a clone of nirsevimab – a mab (see above)
Apart from the UK, most other countries have recommended AZ-Sanofi’s nirsevimab for all new born babies. Unless Merck introduces loss-leading prices it will struggle to find a place in the market. And it is due to be approved by the FDA this month.
Clesrovimab comes as a single 105mg (sic) syringe whereas nirsevimab has 50mg and 100mg options according to the baby’s weight.
The implications of this are that tiny preterm babies under 5Kg and going to be injected with relatively more mab.
Merck boast about this here
https://www.nature.com/articles/s43856-025-00807-9
Showing how serum neutralizing antibodies will be much higher than those induced by Abrysvo maternal vaccine, and even higher in the tinier babies.
More is not better – in most other fields of medicine the aim is to find the lowest dose of a drug that is effective, as most side effects are dose related.
Many journals have spin off cash cows – this is out of the well-known Nature stable. From Merck’s point of view it’s a no-brainer way of advertising, just £2690 for open access.
Suggesting that this product is better for tiny premmies is outrageous nonsense.
Peter Selley says
Who knew that these MABS not only have antibodies, but they also affect the prevailing viruses they are supposed to attack.
MSD’s clesrovimab’ label has just been published by FDA.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/761432s000lbl.pdf
As I understand it – see the section on page 7 – “Antiviral Resistance – in clinical trials”
Resistant RSV viruses were detected in about 8 times as many immunised babies compared with controls, and were associated with a couple of breakthrough infections and some highly clesrovimab-resistant viruses.
The other deeply concerning revelation is that it confirms that there is no dosage reduction for really tiny babies, 105mg for all.
This just does not make sense. It is lunacy.
annie says
June 25 (Reuters) – The U.S. Centers for Disease Control and Prevention’s revamped vaccine advisory panel on Wednesday postponed its vote on the use of respiratory syncytial virus therapies to Thursday.
The panel, which has convened for a closely watched two-day meeting, was discussing the use of AstraZeneca (AZN.L) and Sanofi’s (SASY.PA) Beyfortus and Merck’s (MRK.N) Enflonsia.
US to stop financial support of global vaccine alliance Gavi, health secretary says
https://www.reuters.com/business/healthcare-pharmaceuticals/us-stop-financial-support-global-vaccine-alliance-gavi-says-health-secretary-2025-06-25/
Other donors, including Germany, Norway, and the Gates Foundation, have already pledged money in recent days for Gavi’s future work.
UK partners with Gavi to help save up to eight million lives by 2030
https://www.gov.uk/government/news/uk-partners-with-gavi-to-help-save-up-to-eight-million-lives-by-2030
Secretary Kenned@SecKennedy7h
In its zeal to promote universal vaccination, @gavi , the Vaccine Alliance has neglected the key issue of vaccine safety. When vaccine safety issues have come before GAVI, it has treated them not as a patient health problem, but as a public relations problem.
During the COVID-19 pandemic, GAVI partnered with the World Health Organization to recommend best practices for social media companies to silence dissenting views and to stifle free speech and legitimate questions during that period.
GAVI should consider the best science available, even when that science contradicts established paradigms. It should define success not just in terms of the number of vaccines delivered, but on their rigorously measured overall impacts.
I call on GAVI to re-earn the public trust and to justify the $8 billion dollars that America has provided in funding since 2001. Until that happens the United States won’t contribute more to GAVI. Business as usual is over.
Peter Selley says
Bad timing
June 25 Lancet online first (with the usual cast of characters)
How Gavi support for RSV immunisation will advance health equity
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)01117-1/fulltext?rss=yes
This is full of references to the fact that RSV immunisation COULD save lives – for which there is no evidence.
From the WHO’s point of view Malaria is a bigger problem.
tim says
Thanks Peter,
Just watched Lancet Multimedia: Global Health. September 9, 2024.
Respiratory Syncytial Virus.
Lancet Videos.
annie says
CDC vaccine advisers recommend Merck’s RSV therapy for babies
The vote was the first for the new members of the committee, who had been handpicked by health secretary Robert F. Kennedy Jr.
https://www.statnews.com/2025/06/26/cdc-acip-merck-rsv-monoclonal-antibody-enflonsia/
A committee that advises the Centers for Disease Control and Prevention on vaccines voted Thursday to recommend the use of a new monoclonal antibody against RSV in babies, Merck’s Enflonsia.
The monoclonal antibody, given to babies under 8 months of age entering their first RSV season, is the second product of this kind to enter the market, joining Sanofi and AstraZeneca’s Beyfortus in the RSV toolkit.
Enflonsia was approved by the Food and Drug Administration in early June. At the time, company officials said Merck planned to start taking orders for the product in July and would deliver the doses in the U.S. this fall, in advance of the start of the RSV season.
Kennedy’s US vaccine panel votes in favor of Merck’s RSV antibody drug
https://www.reuters.com/business/healthcare-pharmaceuticals/us-cdc-panel-votes-favor-mercks-rsv-antibody-drug-2025-06-26/
Panel votes 5-2 in favor of respiratory syncytial virus antibody drug, Enflonsia
Panel’s meeting faces scrutiny following Kennedy revamp of panel
One focus of meeting is use of thimerosal in flu vaccines
June 26 (Reuters) – U.S. Health Secretary Robert F. Kennedy Jr.’s newly revamped vaccine advisory panel voted on Thursday for recommending use of Merck’s (MRK.N) RSV antibody drug for infants 8 months or younger whose mothers did not receive a preventive shot during pregnancy.
The panel voted 5-2 in favor of Merck’s respiratory syncytial virus antibody drug, Enflonsia.
It also unanimously voted for Enflonsia to be added to the CDC’s Vaccines for Children program that provides vaccines and therapies free of charge to those without insurance.
annie says
Watch here: The CDC advisory panel on the RSV debate on approving clesrovimab
https://childrenshealthdefense.org/defender/acip-cdc-vaccine-panel-recommends-merck-rsv-shot-all-newborns/
It lasts exactly one hour.
Peter Selley may be the one to pick it apart.
annie says
The CDC advisory panel on RSV was compelling watching. There was an emphatic YES vote in favour.
RSV Vaccines for Children: Still Crazy After All These Years
Vaccine-enhanced disease raises its ugly head again. When will they ever learn?
https://www.malone.news/p/rsv-vaccines-for-children-still-crazy
The bottom line is that there is not a clear, compelling clinical need for an RSV vaccine for children- who have universal immunity, let alone for neonates. Why should we continue to pursue clinical testing of these products in neonates when every child enrolled in such clinical trials will be at risk of VAERD due to some poorly understood mechanism? This has all the hallmarks of another example of an industry that has become enthralled with its own narrative of the power of its technology to solve all related infectious disease problems, and is willing to pursue every potential indication and market opportunity at the expense of humanity.
If I were the incoming Director of CDC or Commissioner of the FDA, I know what I would do about this. I would just say no.
Peter Selley says
Well, Annie, the ACIP meeting was a bit of a farce. Clearly the new panel didnt know what they were doing and had many technical problems. This was mainly about getting Merck’s clesrovimab approved. One of the few members who talked sense was Retsef Levi who knew the facts. There wasn’t much debate.
Robert Malone was strangely authoritative about what a wonderful job the RSV Workgroup had done and that they must be right. Levi’s points about twice as many deaths compared with palivizumab, no long term studies, neurological adverse events and a single dosage for neonates of any weight were ignored.
The approach seemed to be “clesrovimab is no worse than nirsevimab and that was approved so we should approve clesrovimab”. Merck are going to find it difficult to break in to the A-Z Sanofi-controlled market for RSV monoclonal antibodies. By a strange quirk of fate both products cost $556 a dose.
Sadly, RFK Jr’s Dream Team lacked lustre.
annie says
ACIP Debrief- June 2025
With a focus on and explanation of the RSV antibody recommendations
https://www.malone.news/p/acip-debrief-june-2025
Robert Malone comments regarding the RSV decision
There has been some confusion concerning the nature of the product and the rationale for the decision regarding Enflonsia (clesrovimab). I hope the following will help clarify these issues. Note that this represents a personal opinion, and does not represent the position of the Centers for Disease Control and Prevention (CDC) or the US Government.
Let’s begin…..
Why is there no significant concern that using these monoclonal products will select for new RSV viruses that are resistant to these antibodies? Because most of the RSV infections are happening in children and adults who are not treated with these products. So this is a very different evolutionary scenario from where everyone is being dosed with a leaky vaccine, such as happened with the SARS-CoV-2 situation.
I hope that the above helps you to understand the decision, to appreciate that the new ACIP team takes these matters very seriously, and that there was robust discussion and examination of all options as well as the risk/benefit considerations before making this recommendation.
Peter?
Peter Selley says
Meaningless Malonespeak:
“And to be truthful, the risk of hospitalization or death from RSV, even in newborns, is only about 2-3 out of every 100 (2-3%).”
There is absolutely no evidence that MABs prevent death in babies.
The children who were ill/died from RSV VAERD in the Lot 100 trial in the sixties and more recently in Panama were older, so the “logical” discussion about the size of the airways in newborns doesnt stack up.
“Why” he asks “is there no significant (?) concern that using these monoclonal products will select for new RSV viruses that are resistant to these antibodies?”
Well there is significant concern,.
It doesnt take a rocket scientist to predict what would happen if children, sick from these resistant viruses, get admitted to paediatric wards full of other kids who, even if they have had the shot, will not be immune to the resistant RSV.
Malone is a menace.
annie says
This is what Robert Malone thinks of himself.
Top-flight people supported Robert Malone. Especially during the Covid pandemic. Read the ‘heroic’ endorsements from figures such as Robert F. Kennedy Jr. and Senator Ron Johnson regarding his book at the end of his narrative.
https://www.rwmalonemd.com/history
He did cut quite a divisive figure during Covid, but so did Kennedy and Johnson, who were battling against the odds. But this was all to do with Vaccines and not monoclonal antibodies.
“I have never worked on developing any of the childhood vaccine products.”
“I do think that the childhood schedule for vaccines has become bloated and too many vaccines are being given to our children at way too young of an age. The hepatitis B vaccine being given at birth and influenza vaccines being given to healthy children are prime examples of the perversion of the childhood vaccine schedule.”
I must admit my first thought when I saw Robert Malone as a CDC Panel member and now upgraded in seniority, was that this could set the cat amongst the pigeons for all those hurling bricks at the new CDC panel.
Of all the new panel members, I wondered if Robert Kennedy had made a mistake with Malone.
He seems to have cultivated a figure of ‘elder statesman’ in his manner, does Robert think he is a ‘national treasure’.
His RSV bullish chicanery against Retsef Levi and his admirable stance gave a voice to alarm, that for all his fighting talk he may have got it wrong on MABs as Peter has put so well.
With nobody really on the ball except Retsef Levi, it does make you wonder if all the insults Robert Kennedy Jr. received about his new CDC panel needed to let a drug through. After all, if there is already a drug on the market, what’s wrong with another one. They had all made up their minds and with that achieved, batted it off to the RSV pie in the sky.
Peter Selley says
[revised]
UNSAFE SAEF
A Serious Adverse Event (SAE) is defined as any expected or unexpected adverse event, related or unrelated to the therapy being studied, that results in:
Death, a life-threatening adverse event, requires inpatient hospitalization (not required as part of the treatment) or prolongation of existing hospitalization, a persistent or significant disability or incapacity….
Not trivial then.
For the RSV monoclonals injected into tiny babies both companies proudly claim that the SAEs in the two groups are numerically similar – there are no more SAEs in the immunised babies compared to the placebo group.
Merck says its trial of clesrovimab in healthy preterm and full-term infants (Protocol 004) has “a safety profile that is generally comparable to placebo.” Indeed, the incidence of Serious Adverse Events is similar in vaccinated and placebo groups, 11.7% vs 12.6%.
In the Melody trial of nirsevimab, SAEs were reported in 67 of 987 infants (6.8%) who received nirsevimab and in 36 of 491 infants (7.3%) who received placebo.
In these clinical trials a RSV infection was considered as a SAE (in the same way as a seizure or gastroenteritis, or a death) if it fitted the definition above.
Although there is a slight reduction in serious RSV infections in the immunised group, this is balanced by an excess of other SAEs associated with the immunisation product, particularly seizures and infections.
This exposes SAEF – the Serious Adverse Events Fallacy
All SAEs will require a significant budget as by definition almost all require hospital admission.
Hence the fallacy – there is no benefit if both groups have a similar incidence of SAEs, as the companies correctly claim.
Sales of AZ-Sanofi’s nirsevimab reached $1.8 billion in 2024.
The serious money being spent by governments will have minimal impact on overall hospital admissions of immunised babies.
Peter Selley says
Interview with ACIP member Retsef Levi, explaining why he voted against the approval of clesrovimab in babies.
https://brownstone.org/articles/retsef-levi-explains-his-vote-against-routine-rsv-monoclonal-use-in-newborns/