
The Holy Grail © Nina Otulakowski June 2022
You need to click on the image to get the full effects.
In recent months, RxISK has been working closely with Luisa Guerrini in Milan, whose background is in research on regulatory proteins like p 63 and p 53, on which Thalidomide works. This discovery led to excitement a few years ago when it was thought the mechanism through which Thalidomide causes birth defects had finally been found.
Thalidomide also causes sexual dysfunction and suicidality and these effects overlap with the effects of SSRIs, Isotretinoin and Finasteride which also cause the same problems.
Luisa has since been running assays to test what the effects of SSRIs, Isotretinoin and Finasteride are in the systems on which Thalidomide acts. See The Holy Grail.
Three Experiments
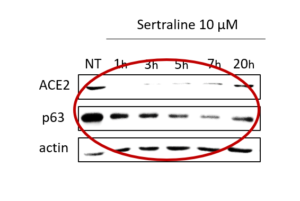
The answer is that there are overlaps. In the first slide you see a steadily increasing effect of sertraline on ACE2 receptors and on p63, with no effect on Actin which is there as a control. Luisa has found the same effects with Isotretinoin and Finasteride.

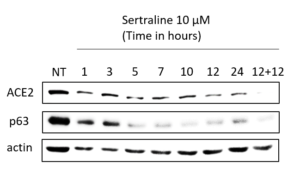
In the second slide you see that the effect of sertraline is very visible for up to 12 hours in fact after which ACE2 receptors and p 63 begin to recover.
Finally in the third slide, sertraline has been added in again at 12 hours in some of the plates and not in others and you can see that the recovery continues from 12 to 24 hours in the plates with no extra sertraline but there is an even more comprehensive wipe-out of ACE2 receptors and p 63 with the second dose of sertraline.
Another hugely encouraging sign is that there are very similar results with both Isotretinoin and with Finasteride. Having common effects across all three drug groups suggests we are on the right path and in addition the goal has always been to find an answer for the enduring sexual dysfunctions that all 3 drugs can cause.
Quiescence
There is more good news than this, however. What happens when p 63 is affected like this? The answer in this case appears to be that cells go into a state of suspended animation. They stop dividing. This again appears to be consistent with what happens in the sexual dysfunctions – things stop working.
The next step is to pinpoint exactly why they stop working Have the powerplants in the cells, the mitochondria, been struck by SSRI or finasteride missiles? Or is something else happening?
Do the cells stay in a state of suspended animation or do they die? Do SSRIs, Finasteride and Isotretinoin all behave the same way or are there points at which they diverge? At the moment, Isotretinoin looks the most potent – the most damaging.
There are other fascinating aspects to this. One is p 63 is the gateway to the neuro-epithilium that forms skin and nerves. This is of interest because SSRIs, Isotretinoin and Finasteride all have effects on skin (hair is a part of skin). Their effects on skin in all three cases are more obvious than any brain effects.
This would also fit in with recent indications that at least some people with enduring sexual dysfunctions have a peripheral neuropathy – see Sensory Receptors and Neuropathy. In the case of small fibre neuropathy we are looking at effects on small nerve fibres in skin.
Thalidomide was also famous for causing a peripheral neuropathy – this was what Frances Kelsey in FDA was concerned about when she delayed the licensing of thalidomide in the United States – not birth defects.
Antibodies
There has been great interest in antibodies lately with many people with PSSD in particular getting test results back showing they have antibodies to Muscarinic, Catecholamine and ACE receptors.
It is complicated to work out what is happening here as COVID and the vaccinations for COVID also seem to cause increases in these antibodies and cause peripheral neuropathy and perhaps an enduring sexual dysfunction as well.
Many of those who get antibody tests post COVID or vaccines have had SSRIs prescribed to them, so teasing out what is happening becomes very difficult. It will be important to keep good timelines as to when the problems began and important to see results from some who have had the vaccine but not SSRIs (or tetracycline antibiotics or antihistamines) or those who have PSSD but have not had vaccines or COVID.
We also need some people to get tests done in laboratories other than Cell Trend, where the majority of results have come from so far. We might even need some of those with results from Cell Trend to get tested in other laboratories also and see if we get the same results back.
The reason to mention this is these results are very important and we need to be absolutely sure what we are dealing with.
Finasteride MetaboTypes
A paper just out in Nature Medicine introduces a new idea – Metabotypes. It appears we differ in how our metabolisms respond to finasteride – we split into different groups. This raises the possibility that one of these Types underpin suicidality on this drug or enduring sexual dysfunction. At present it is not clear if specific genes underpin these Types or whether it will become possible to pick out those of us who can take finasteride safely and those who should avoid it.
Merck should be interested in this and should help fund research to find answers to these questions but their response is more likely to be the same as the Tobacco Industry – who have put no effort in tracking down who might be able to smoke with impunity as this would likely reduce their market size and also help confirm that finasteride/tobacco has a role in causing certain problems.
Clinical Trial
A possible treatment for PSSD, PFS, Post Isotretinoin syndromes and Enduring Withdrawal Syndromes has emerged. We are awaiting results of a clinical trial currently in progress to see if a trial in PSSD makes sense. At present the prospects look good.
While this will be welcome news, and it is welcome news, people should not get too hopefuly too quickly. There will be no quick answer from a clinical trial – there never is.
There will be no large drug company behind this trial of an old drug. So getting a trial to happen and rolling anything that works out to people will need support. Keep an eye on RxISK posts for updates.
Equally, there is no large drug company willing to pay the fees to make Luisa Guerrini’s papers open access – and available to everyone with PSSD, PFS and Post-Isotretinoin Syndromes. We welcome all contributions to help support her work which involves having to order specialized antibodies from China.
The funding Luisa has been given at present is for one Post-Doc for a year. When the work began we had no idea that it might develop as well as it has. The good side to the progress made is we have novel findings now being written up and these will hopefully generate wider interest and the involvement of others.
Sarah Browne says
What promising research! If it turns out that SSRIs, finasteride and isotretinoin all exert their enduring sexual side effects via a mechanism similar to that of thalidomide, then this makes the failure of pharmacovigilance surrounding PSSD, PFS and post-retinoid syndrome all the more shocking. The Yellow Card Scheme was set up after the thalidomide scandal so that adverse reactions could be monitored and we could be safe. The failure of Drs to listen to their patients and report these events shows a disregard for the reason the Yellow Card scheme came to be…
José Miguel says
Gracias por su trabajo
Me llamo José Miguel y estoy muerto en vida por pfs desde hace 6 años.Lo he perdido todo y simplemente decirle que estaría dispuesto a prestarme en cualquier estudio.Mi caso es muy extremo
Gracias
Arjan says
https://pubmed.ncbi.nlm.nih.gov/34602110/
Impact of ACE2 genetic variant on antidepressant efficacy of SSRIs
Sufferer says
I am pretty sure that the reason accutane stops cells from dividing is discovered? It makes the cells divide so fast that they cant repair and cant divide anymore because of telemore shortening. Why dont you just test the chromosomes on the sebaceous glands and see if i am right or wrong? It offers no hope however as there is no current cure for aging. Even if there was, fixing cells that are already dead should be impossible.
Dr. David Healy says
We can check this but interestingly in the Milan cell system at a lower dose it causes a pause in cell division as sertraline does. Increase the dose of both and the cells die. We hope to explore this further.
There will be a post next week and these issues and it would be good if you can comment with references and further ideas
David
Sandman says
Hello Dr Healy
I currently have a group on reddit of 100 pssd suffers. We are currently trying to fund people doing celltrend tests.
Please note we are seeing a few people see improvements with plasmapheresis(blood wash), regarding auto anti bodies.
Please take into account I believe there should be focus on B3-AR which is not shown in these celltrend tests. Which I believe needs testing aswell as it relates to sexual/genital function.
We are trying to find out if celltrend or another place can have this done.
Kind regards
Boost909
Arjan says
it might be a better idea to do same test through other labs to verify accuracy of Cell Trend as pointed out in this article.
Sandman says
Hello Dr Healy
I’m yet to be tested but i will be doing a cytokine panel soon.
I was trying to figure out the similarities between supplement/steroid based recoveries and people who get windows.
I have found most ssri, snri, antipsychotic, other drugs, finasteride, accutane, ashwaganda, including many other herbs are immunosuppressive or over stimulate the immune system. I noticed people would crash due to certain cytokine mechanisms.
I also believe the drug half life has alot to do with the interaction as it’s hard to predict what’s in the persons blood at the time and overlapping supplements when they recovered or improved / crashed.
Also when people where getting pssd some where swapping between multiple ssri, medications or supplements without being fully aware of the drug half life.
I noticed the correlation between covid 19, celltrend results and androgen receptors, gut theory ( gut brain axis ) (hPa axis) all point to one possible underlying mechanism.
Cytokines, which are also made in the gut.
I noticed when people get pssd suddenly stopping from prolonged use or from taking one pill/few or after a heavy night waking up feeling numb i thought it tied in with the cytokine storm caused by covid 19.
I’m not sure how this correlates to ACE2 and the anti auto bodies.
Just that it appears to be a cytokine reaction from the body either rejecting or adjusting to the immune response either being over active in reaction or bouncing back from being suppressed. I believe this is where the point where pssd is caused. ( possible cytokine storm )
I noticed people who made progress with immunotheresis might not be because we are targeting the celltrend auto anti bodies in relationship to bc007. It may be that it’s treating the immune response to cytokines, as they are found through out the body and genitals.
I have found saffron helpful and I’m still trialling it, it’s also known to help covid 19.
Just food for thought!
Kind regards
Boost909
Patrick D Hahn says
So SSRI’s knock out the ACE2 receptor, and SSRI’s lead to sexual dysfunction. That’s … kinda interesting. Guess what else knocks out the ACE2 receptor? The spike protein.
We know the mRNA “vaccines” are having all kinds of effects on women’s reproductive systems. I can find only one study of the effects on men’s reproductive systems:
https://jamanetwork.com/journals/jama/fullarticle/2781360
A study of forty-five men found the mRNA “vaccines” actually increase sperm production. But I’m not sure we can assume that is a good thing. I’d say any alteration in one’s physiological parameters is cause for concern.
Patrick D Hahn says
Just searched VAERS for reports of “sexual dysfunction” for 2021, the first year of the covid vax rollout. There were twenty-one reports of sexual dysfunction. Of these, nineteen were associated with the covid vaccines.
Yes, I know, the CDC tells us that VAERS reports are not considered proof of cause and effect. What they don’t tell us is that the CDC promised to carry out proportional report ratio analysis weekly, and the FDA promised to carry out empirical Bayesian data mining biweekly, and they either haven’t done so, or won’t let us see the data.
susanne says
There’s a lot of interest presently on Reddit and a mention of today’s blog. Will the clinician who will be testing in UK next year for Rxisk be collaborating with Luisa G. in Italy?
I ask because one of the few journals who do publish articles others refuse published a huge amount of detail including many names of those used for reference to their own work and their institutions It’s four years later but would Rxisk and L G. be able to do a follow up article in that Journal even to alert others there is serious progress being made presently ? Perhaps they might think of setting up a dedicated clinic if there seems to be a rewarding project in the air..It is urgent now there is a world wide massive increase in prescribing with all the associated potential harms. Maybe if there was as much emphasis on already proven potential suicide, which was more covered up 4 years ago, could be avoided with testing they might take more notice .
Referred to above – 2018
CiteCitizen petition: Sexual side effects of SSRIs and SNRIs
Authors: Healy, David
Affiliations: Data Based Medicine Americas Ltd.,
DOI: 10.3233/JRS-180745
Journal: International Journal of Risk & Safety in Medicine, vol. 29, no. 3-4, pp. 135-147, 2018
DOI: 10.3233/jrs-180745 PMID: 29733031 PMCID: PMC6004927
and 2022
ArticlePDF Available
Diagnostic criteria for enduring sexual dysfunction after treatment with antidepressants, finasteride and isotretinoin of the Creative Commons Attribution-NonCommercial License (CC BY-NC 4.0). 66 D. Healy et al. / Diagnostic criteria for enduring sexual dysfunction after treatment
January 2022
Project: Eventos adversos y Seguridad del paciente psiquiátrico
Authors:
David Healy
Bangor University
Audrey Bahrick
University of Iowa
Maarten Bak
Angelo Barbato
Mario Negri Institute for Pharmacological Research
Show all 36 authors
and
r/PSSD
u/ImpressiveNet370
2 days ago
My neurologists took this seriously!
I was referred to the university hospital due to severe PSSD and they started a serious hunting. I met the medical director of neurology department and several neurologists. They all say that I am most likely suffering from a severe autoimmune condition and they are still performing a full body-CT (due to endothelial and vascular dysfunction), lumbar puncture from cerebrospinal fluid with all possible neurological antibodies (including all possible encephalitis). They also investigated my positive results from CellTrend and it became clear that these results really matter in my case. It was also stated that the “research” claiming that CellTrend results can be positive amoung normal people was based on false analyzes (high risk values were interpreted as positive just as real positives – so they mixed them). Anyhow all my symptoms are autoimmune related and still investigations take place before an immunology meeting is organized and they will decide about best possible treatments. It’s clear that I have a neuroinflammation together with autoantibody mediated circulatory dysfunction and SFN.
I keep you all posted.
Renato says
Susana,
Good afternoon!
Please keep me informed. I’ve been suffering from this for 3 years and here in Brazil, we don’t have anyone looking at it.
I will be forever grateful if you can tell us your results.
Hug!
susanne says
Maybe members of PSSD will have useful information Posted by
u/escitalopramsucks
3 months ago on Redditt
Dra Luisa Guerrini is researching PSSD.
Dr.Luisa Guerrini Who is nowadays researching PSSD, is asking us to answer a simple question. Have we ever had Covid or not?? Please, try to answer the questionary as this is something she needs for her research. Passed is.incorrect, sorry, I meant if you ever HAD Covid
155 votes
6
3.9%
Passed Covid not vaccinated. Serious symptoms
31
20.0%
Passed Covid not vaccinated. Mild symptoms
52
33.5%
Passed Covid vaccinated. Mild symptoms
16
10.3%
Not passed Covid. Not vaccinated
37
23.9%
Not passed Covid. Vaccinated
13
8.4%
Passed Covid vaccinated. Serious symptoms
Voting closed 3 months ago
42 Comments
Share
75% Upvoted
Sarah Browne says
I did not respond to this questionnaire as I didn’t see it. I was vaxxed and got Covid. It was ridiculously mild and I only bothered testing I had been sharing a room with someone who subsequently tested positive. Does Dr Guerrini suspect that PSSD patients are less likely to get Covid or get milder disease as a result of reduced ACE2?
Dr. David Healy says
No one knows the answer to this yet. There are all sorts of interesting angles on these things that this research program might bring to light.
D
Matty says
I have PSSD after SNRI Duloxitine between August 2019 and May 2020. It started before covid pandemy has begun. I live in Poland where No doctor listens to me and others about PSSD. Please inform me about new tests and discoveries. Best regards! Matty
Dr. David Healy says
Mattie
Keep reading RxISK posts for updates
David
Darman says
I cant say I fully understand this but it does offer hope. It would be nice to know what possible treatments are worth perusing with these results in mind.
Dr. David Healy says
No one fully understands this. Not even Luisa understands what is going on. This offers an opportunity rather than a dead end – and offers an opportunity to you and lots of other to read up about these things and see if you spot possibilities that at the moment no-one else spots. Luisa has the opportunity to test things and see what happens – which will hopefully steer us down one of the many paths that seem possible at the moment
David
mary H says
ANY good news is worth shouting about these days in my opinion. Small steps always better than massive leaps too. Having said that, now may be a great time to do our best to boost the Research Fund where “massive leaps” would be welcomed, I’m sure!
Darman says
Thank you for your reply Dr. Healy. I am doing everything I can although not being in the medical field I have little to go on other than anecdotal reports of recovery and possibly mechanisms. Currently I’m looking into gut health etc. to see if changes there can perhaps improve things.
It’s good to know as least some professionals take this seriously and are investigating it.
Many thanks
ben says
I urge everyone with PFS to get tested for mycotoxins.
You may have been living or working in an area with a high mycotoxin load and finasteride was the loaded gun to increase your toxic load and stop your detox pathways as it blocks glutathione. Then you would see the damages from mycotoxins, including dopamine pathway issues, adrenal, neuro, hormonal issues, gut health issues, its a cascade that shuts down most biological functions.
These mycotoxins will remain in your system until you specifically target and bind each type.
ben says
How can we follow this work as it progresses?
Dr. David Healy says
Rather than follow you and others can engage in the research by exploring everything you can about SSRIs and p 63 and ACE2 receptors, cell cycles and mitochondria – and the same for finasteride and isotretinoin. This is not a time to sit back and follow – if not chasing the literature find out who is doing research on p 63 and draw this to their attention and perhaps get them engaged in replicating and adding to these early results
D
Sam says
How can I support this research? it looks encouraging bus is far above my head. Can someone explain what type of experimenting we can do ourselves to help this?
Dr. David Healy says
See reply to Ben about bringing the preliminary results to the attention of others engaged in research on p 63 and ACE2 receptors – these may be COVID researchers who know nothing about SSRIs and PSSD or isotretinoin and finasteride. All the better if they become aware that there might be aspects to their work they didn’t know about
D
low_water says
I myself had had long Covid (full ME/CFS).for about 3 months before I got PSSD from ashwagandha (one pill only), 4 months ago. There must be a link for I’ve seen many similar cases.
Why don’t any of us contact the lead scientists in the polybio.org consortium – the leading scientific innitiative working on long COVID and suggest any link.there might be between LC and PFS/PSSD to them?
If there’s an identifiable link between PSSD and LC, our community would profit from the LC research momentum (10 billion allocated as of 2024 for LC for 10 years, by senator Bernie Sanders.. and so much media traction).
Dr David HEALY should undertake that communication himself. Where on Earth have we seen patients financing the research, let alone doing it? I mean what is that?
Scientific discoveries don’t happen just by chance. They happen when they’re (decently) financed, like they were for HIV or cancer (in fact, scientific discovery is deterministic in nature : scientists will find the answers, if there’s appropriate finance, and not until there isn’t).
And they happen thru heavy collaboration between scientists. Not from one single lab.
They don’t happen by trial and error from patients – or even doctors. HIV wasn’t solved by trying supplements and unpatented drugs. And plasmapheresis worked only as a patch until decent therapy appeared around 1997 (the tritherapies).
If we agree PSSD is a serious disease it’s about time we – sufferers and the few experts – started treating it as such.
Sean says
Thank you Dr. Luisa Guerrini for looking into this horrific condition. It is so refreshing to see professionals who actually want to help us instead of leaving us alone in this darkness. Thank you.
Dr. Tom Lue says
Hi there, I love this article!
The news that a potential treatment may be on the horizon for PSSD, PFS, Post Isotretinoin syndromes, and Enduring Withdrawal Syndromes is welcome and exciting.
It’s great to see that despite no large drug company behind the trial of an old drug, the prospects still look good.
Furthermore, it’s admirable that Luisa Guerrini has been given funding for one post-doc for a year to carry out her work.
I appreciate the encouragement not to get too hopeful too quickly, as clinical trials take time with no quick answers.
Moreover, I like how you highlighted the need for support to make Luisa Guerrini’s papers open to access.
This will enable more people to benefit from her work and, in turn, make a difference in patients’ lives and their families.
Luisa Guerrini has been able to make significant progress despite the lack of investment from large drug companies.
We, as a community, must rally around her and support her research by donating financially or offering our skills and expertise where we can.
Seeing how far she has come in such a short time with limited resources is inspiring. Hopefully, this encourages more researchers to pursue similar projects without fear of failure.
Overall, the article was very informative and uplifting.
Thank you for sharing!
susanne says
It was great to read Tom Lue’s encouragement comment so clicked on Tom L’s name on the top of his comment. It took me directly to an advert for the treatment for sexual problems but there’s no suggestion he is using the blog to advertise this private business which concentrates on treatment for erectile dysfunction There is though good evidence of his decency and willingness to speak publicly about pharma;-
This is the advert if click on Dr Tom Lue on comment –
Levitra online storeBestsellersFAQPoliciesContact Us
£0.90
Levitra
Vardenafil 10/20/40/60mg
Vardenafil is used for treatment of erectile dysfunction. It assists men in achieving and maintaining an erection during sexual activity. Vardenafil is marketed under the Levitra trade name. Our site offers the original, Brand Levitra and it’s generic version, which consists
Levitra
Generic Levitra – a drug designed for men with a reduced erectile function and sexual…
our price
£0.90
Buy Now!Levitra®
Levitra® is a medciation for the treatment of male Impotence manufactured by Bayer…
our price
£8.97
Buy Now!More ED drugs »
GET FREE SAMPLE
TABLETS WITH YOUR ORDER
Special Offer!
Levitra online storeBestsellersFAQPoliciesContact Us
Click on information on their website
News
How Big Pharma’s Shadow Regulation Censors the Internet
Sat, 05 Aug 2017 09:37:41 +0000
In the US most prescription drugs have the highest prices in the world. And get benefits from this state of affairs certainly big pharma, in their interest to leave things as they are. For most Americans the access lower-priced drugs from overseas is unlawful because of such documents as the Prescription Drug Marketing Act and Ryan Haight Online Pharmacy Consumer Protection Act together with the powers of U.S. Customs and Border Protection (CBP) to seize such drugs at the border.
But in fact, American consumers are allowed to import a 90-day supply of some prescription medications for personal use by bringing them from abroad or ordering and mailing them from overseas, by discretionary guidelines developed by the Food and Drug Administration (FDA) and enforced by the CBP. So there is a huge market for pharmacies registered outside US such countries as Canada, Australia and Turkey that accept online orders and mail genuine pharmaceuticals to American consumers at much cheaper prices.
Big pharmaceutical companies are not satisfied with this, but they can’t do much more about it as the importation of medications is already technically against law. They can’t do that legally as they can’t get government to regulate the Internet in the way they want. So big parma uses so called Shadow Regulation with Internet intermediaries attempting to quell the supply of prescription drugs to American customers via overseas online pharmacies.
This regime of private censorship in the Internet includes blocking and blacklisting pharmaceutical websites from access to online advertising services, payment services, domain names.
Profile of a Shadow Regulation Network
The Shadow Regulation network includes three key players: the Alliance for Safe Online Pharmacies (ASOP), the Center for Safe Internet Pharmacies (CSIP) and LegitScript. The first one is comprised mostly of the pharmaceutical industry, the second one deals with Internet platforms (Facebook, Google, Microsoft and Yahoo!), delivery providers (UPS), payment processors (PayPal, MasterCard, and American Express), and domain registration companies (GoDaddy and Rightside), and the third one played an important role in organization of both ASOP and CSIP and implements most of the arrangements. An interesting fact that Internet users whose rights they protect are not represented at board level in any of these organizations.
Usually the governments also take part in this Shadow Regulation and here we have the same situation. White House announced the formation of the CSIP on October 14, 2010, after several months of negotiations between the administration and the founding members of CSIP. LegitScript headed by former Associate Deputy Director Office of National Drug Control Policy, and subsists on profitable contracts with the government. So having such framework is very easy to defend the interests of the pharma industry affecting Internet intermediaries.
Internet Blacklists
There are only two registers of online pharmacy websites are approved by both the ASOP and the CSIP. They obey LegitScript and by theNational Association of Boards of Pharmacy (NABP) under the name Verified Internet Pharmacy Practice Sites(VIPPS), and not only exclude sellers of fake and counterfeit drugs from their approved lists but also exclude overseas online pharmacies that supply genuine drugs to Americans under the FDA’s personal use policy. In such a way they prevents American customers from even findingonline pharmacies who can fill prescriptions inaccordance with FDA policy. Such online pharmacies are blocked from access to essential Internet intermediaries such as domain registrars, payment processors and online advertising networks.
Within the framework of this Shadow Regulation regime new top-level domain .pharmacy wasgranted by ICANN to the NABP last year, despite the fact that there was petition from users opposed with almost 25,000 signatures.
The NABP is demanding ICANN force domain registrars to require from any pharmaceutical website a license to distribute medicine to any jurisdiction that it ships to. This demands would wipe online pharmacies off the Internet altogether.
The opinion of of healthcare consumers and Internet users were not taken into account, because it is not profitable for the powerful government and private industry forces. All these measures were taken to favor the private interests of big pharma and to limit access to information and access to safe and affordable medicine.
We can’t deny that fake and substandard medicine sales are a problem that should be regulated by law enforcement agencies. But they should do that legally through cooperative mechanisms that are inclusive, balanced, and accountable.
All products:………..below on website
Dr. David Healy says
Susanne
Thanks for pointing this out. I was so pleased with a supportive comment that I didn’t look any further. In general anyone advertising their wares in a comment doesn’t get posted.
David
Andrew says
Hi Dr. Healy,
This is a fascinating find, thanks for sharing!
A bit of cursory reading on ACE2 led me to find out that one of its major roles is to activate endothelial nitric oxide synthase (NOS) via its enzymatic product angiotensin(1-7); this seems like it could be highly relevant to PSSD, given NO’s role as a neurotransmitter, and specifically as a major player in erectile function. Do you or your team have any thoughts on this as a potential mechanism for PSSD, or at least a contributor?
Dr. David Healy says
Andrew
All ideas like this are good to hear about. The great thing about this research is it will be possible to chase these leads – although chasing all of the ones that have come our way since the post will take time.
I have to say this is perhaps the most exciting research that I’ve ever been involved in – fingers crossed
David
tim says
The last 32 years in my lifetime of clinical medicine included an ongoing research commitment. At times this was intensely rewarding academically.
My response to the research recorded above was that it is amongst the most exciting research that I have read.
I wish you and your colleagues every continued success in this vital work during, and throughout the New Year. Congratulations and sincere thanks to all contributors.
Sandman says
Hello Dr Healy
In relation to my previous posts here is a link: https://www.potomacpsychiatry.com/blog/depression-bipolar-anxiety-mental-health-genes
I have spoken to the duty Scientist regarding tests.
I believe pssd has to do with the cytokines, methylation, SLA6a4 Gene, MTHFR Gene, possibly how it affects 5ht2a and nNoS.
Ssri impact on IL-10 / ifny regarding nb-kB function. After (cytokine storm).
Cytokines downstream impact on methylation (MTHFR) to SLA6a4.
I’ll continue to research ! Unsure how this impacts ACE2 and P63.
Also would you be able to indicate any timeframe regarding the new trials your doing please.
Kind regards
Boost909
Dr. David Healy says
Very hard to specify a time-frame. I am hoping for significant developments next year
David
susanne says
David
– Do you think the research will cross over to understanding the effects of other/most/all drugs?
Dr. David Healy says
hard to know
D
Arjan says
Thanks for this great post!
We all really appreciate your and colleagues efforts shedding light on our horrible condition
What’s the reasoning behind not mentioning what medication it is?
Have you searched the pssd/pfs forums and subreddits on if they’ve been tried by sufferers?
Also would you expect it to be a one-time cure or a regular treatment? I ask this since you’ve used the word cure in the title and treatment in the article
Sandman says
Hello Dr Healy
To keep it brief:
Referring to my previous post on cytokines.
I will be pushing our group towards doing complement system tests.
I believe the compliment system in control of cytokines and phagocytosis may be a great marker for pssd.
I feel this is important!
Kind regards
Boost909
drman says
hello dr healy. can i ask can this work on ppl with people pssd from antipsychotics one example abilify?
Dr. David Healy says
If this works for anyone, we will be much closer to an answer for everyone
D
Mark says
Would this mean that blood pressure meds or ace inhibitors would help with this?
https://www.the-scientist.com/news-opinion/blood-pressure-meds-point-the-way-to-possible-covid-19-treatment-67371
Dr. David Healy says
No one knows – it may be that people on ACE inhibotors or ARBs don’t develop this problem
If someone has access to a big database they could find this out
Might also be good to get a message out on Reddit or whatever
– if you started on an ACE inhibitor or ARB/sartan and your PSSD/PFS/PAS cleared up can you let us know
D
shadowman says
I took Losartan while on SSRI (at the time when I was ok), while SSRI (when sexual problems started), after the SSRI (when I developed every kind of symptom), I stopped taking it, then I took for a time more, felt no difference apart from some kind of rash, a itchyness on my skin, which resolved after stopping the drug. My skin gets red very easily on touch, this never went away.
I dont know if its related but, I think that my first symptoms(the sexual ones) started a year or so after adding Losartan to the mixture, I remember the bad bouts of itchiness during that days, who lead me to a month of antihistamines. Prior to Losartan I was prescribed with Acetazolamide. I think if this contributed with something, since I have nasty NAT2 SNPs.
But I dont know, since my brother whos on SSRIs too, just began developing symptoms(not sexual, but sleep problems, metabolism like high insulin, restless legs…). He developed some king of attention/focus problem after covid.
Just wanted to share my experience with an ARB drug.
Dr. David Healy says
This is great to get. Thanks. It would be good to get as many reports as possible of people taking ACE inhibitors or ARBs – also called Sartans – pointing to making withdrawal or PSSD worse or making them easier.
DH
August says
Dr. Healy – What is the drug in clinical trials?
Dr. David Healy says
there is no drug in a trial for PSSD at the moment
There is other research going on the outcome of which may point a way forward
D
August says
Yes sorry, I meant the drug you mention here:
“We are awaiting results of a clinical trial currently in progress to see if a trial in PSSD makes sense.”
What is that trial?
Dr. David Healy says
its not a trial of PSSD. What I am interested in are trials in peripheral neuropathy
D
Sandman says
Hello Dr Healy
In my research I would like to add further information.
Regarding: Complement system, phagocytosis, cytokines, methylation, possible organic acids and mycotoxins.
I’m leading towards cytokines and the affect of methylation on the body as we see people getting full windows with L-Histidine.
My focus is still looking on IL-10 IL-6 and ifny and tfna.
Focusing work around prok2 and PROKR2 I believe checking genes or function of IL-1a and IL-1b would be important.
I’ve noticed from researching recoveries stories. That things from inositol and flagyl antibiotics and many supplements affect cytokines IL-1B and Nf-kB.
You will find IL-1b as an important factor in LPS and SFN and possibly a marker behind pssd.
Kind regards
Boost909
Sandman says
Hello dr Healy
I have a pssd group of 100 people. Originally we were pushing people through celltrend but trying to get others to do the tests through other labs.
Regarding auto anti bodies and ACE2.
Im looking at GnRH neurons and wonder there impact on the situation. Possibly testing gnrh or lh response to gnrh ? Regarding prok2 and prokr2.
I’ve researched the impact of The complement system and phagocytosis and cytokines IL-a and IL-b and Nd-kB. Would a cytokine and methylation panel be of any interest ?
We have had someone in the group see results with FMT and immunotheresis and Another member getting immunotheresis in feb next year. What is your opinion on immunotheresis and cytokines ?
Should we test the following genes and if so what are we looking for ? There turned on/off, mutated, or if we are suceptible ? p53, p63, p73.
Would sla6a4 be any indicator to our serotonin system or mthfr yo methylation?
Please let me know what I can do regarding testing, what you feel the most important tests are and I’ll pass it onto 100 other members of the pssd group and we will focus on getting you the data you need.
Just so we are spending the money we have on the right tests on data that would be valuable to your research instead of shooting in the dark.
My understanding is your researching is covering a lot of topics p53, p63, p73 and prok2 and prokr2 and ACE2. Would you lean towards these being your main focus ?
If so once again what tests do you want, if celltrend would it be important for everyone to test ACE2 ? Would you like gene panels done to those specific genes ? Just guide us in the right direction and we will get you the data you need.
Kind regards
Boost909
Dr. David Healy says
You’re asking questions that no one has the answer to – if I had the answers there would be no need to ask the questions. The problem for everyone is there are so many elegant theories that can be built about what is going on – the thing that counts is not the elegance of the theory but its testability and also where possible building backwards from things that seem to work to establishing how it might be working
D
Sandman says
Based on your current research and direction what tests could we do to get you more data ?
Dr. David Healy says
At the moment, these are not answerable questions
D
Hope says
Hello Dr Healy, if a drug works on genital anesthesia, will this work also on emotional blunting ?
You talk about clinical trial with an old drug. Is it a trial on ACE And p63 ?
Thank you.
My last hope is your research.
Dr. David Healy says
if something works for genital anesthesia, my hunch is it will work for emotional blunting also
D
Hope says
Thank you for your answer.
I took L tyrosine in order to improve my PSSD but it clearly worsened it. It took the last emotions I had left And worsened pssd also.
I dont understand how an amino acid can do that. Is it related to ACE And p63 ?
Also can you explain why we dont feel tiredness ? And since this I never got sick although before I was often sick with common cold for exemple.
H.C says
Dear Dr.Healy,
I have a few comments/questions regarding the experiments :
You say, “In the first slide, you see a steadily increasing effect of sertraline on ACE2 receptors and on p63, with no effect on actin which is there as a control.” This somehow suggests (although not explicitly stated) that if the ACE2 receptor or p63 line fades, while the actin line remains the same, it means that sertraline has mediated this effect. The control (actin) only shows that the observed wipe-out effect is not from experimental handling, since its concentration should remain constant (assuming sertraline has no effect on actin). However, the control used here (actin) does not allow one to conclude that the observed wipe-out effect is mediated by sertraline. In fact, on the first slide (and only on the first slide not the other one) the first column of the electropheresis should be compared to the other columns to deduce that it is mediated by sertraline. Taking this into account, we see a wipe-out of p63 (comparing the first column and the others) but the wipe-out of ACE2 receptors is not striking if not non-existent.
On the second slide, you assume that the wipe-out over time is due to sertraline. I don’t see how you come to that conclusion. You would have had to perform the exact same experiment without sertraline and observe that ACE2 receptor or p63 do not fade over time. This would have proven that the wipe-out of ACE2 receptor or p63 is in fact due to sertraline. The fact that there is no actin fading while there is fading of ACE2 receptors or p63 does not mean that this is due to sertraline, for the same reason discussed above.
The same remark can be made for the third slide. The exact same experiment would have had to be performed without sertraline to conclude that the wipe-out effect is mediated by sertraline. The fact that the wipe-out effect seems more pronounced when sertraline is added again at 12H suggests that it is mediated by sertraline but it is not definitive that no other factor (experimental handling…) might explain it.
Is it possible to know what exactly NT means? According to the unit, NT represents a concentration in the first slide while it represents a time in the second and third slide. I assume that in the first slide NT means that there is a concentration of zero while in the second and third slide it means that no time has passed.
I may have misunderstood or misinterpreted some of the results in which case please tell me.
Thank you in advance.
Dr. David Healy says
H
You haven’t misunderstood or misinterpreted – you were given no chance. This post is not a research paper. My hunch waa that people with PSSD etc needed some hope. So these images came from a panel of 16 images which included similar results for clomipramine, paroxetine, fluvoxamine, isotretinoin and finasteride with a legend at the bottom. The full figure makes a little more sense – but even then this figure was an early stage and not the final figure that might go into a paper.
The issues for Luisa and her team are whether to produce a quick and dirty early brief publication to flag up that there is something of real interest here or whether to wait till we understand much more about what is going on and then produce a much more substantial paper. We have been leaning more toward an initial brief publication with a follow up more detailed paper.
There are unquestionably intermediate steps in what we have found. One of the wider research team (everyone with PSSD) has veen emailing in articles on SSRIs and placental or amniotic sac inflammation that can lead to birth defects etc – this may be mediated through p 38 and it is not impossible this plays a part in the sertraline results you see here and this may lead to similar outcomes on p 63 and ACE to the outcomes found with thalidomide and isotretinoin but by a different route.
This is one argument for having an initial publication which reports initial results but hasn’t yet teased out how this is happening. The more researchers become aware of possible findings in this area and think these are worth exploring in more detail the better for all of us.
David
H.C says
I had understood that the purpose of the article was not to present a definitive scientific publication but rather preliminary experimental results or hypotheses. However, one must bear in mind that most people here will not understand the tone of the article and will take it at face value. That is why I have explained why the electrophoresis images do not allow one to infer what is written in the article.
You say that people with PSSD need hope. That may be so. However, hope can lead to desperate and absurd actions and this is what unfortunately takes place in our community. Some people, based on far-fetched or unfounded assumptions, undergo potential dangerous and expensive procedures: plasmapheresis, immunosuppressants… Some testing laboratories, whose business model is to make people believe that they have a test indicating what is wrong with them, take advantage of this to make a profit.
When I look at our community I see mostly lost people who don’t know where to go. Rather than hope, our community needs a lighthouse to prevent them from getting lost. The article here mixes several concepts without really explaining them. It adds confusion.
Recently you reported abnormal biopsy results assessing intra-epidermal nerve fiber density (IENF) in a group of patients. This represents the first robust biomarker for the presence of neuropathy in PSSD patients. However, the communication surrounding these results has been unclear. Many people do not understand what these results mean. They don’t even understand what neuropathy means. They don’t understand that a biopsy evaluating the IENF is a much more meaningful medical test than, for example, a serological test with questionable results and normative ranges. They also do not understand that the presence of certain elevated autoantibodies may be a consequence but not the cause of PSSD. These concepts should be explained or people will not understand.
I am sure you have the best interests of PSSD patients at heart but I think you need to be clearer on some points. This is at least my opinion, I could be wrong.
Sincerely
Dr. David Healy says
Dear H
There are people committing suicide because they have no hope. What exactly are you doing about this?
Sure there are scammers – there are earlier posts on RxISK about this if you care to go back and read them. These posts led to a ton of nasty comments and outright threats.
There is also the RxISK Prize that was set up to let people know that these scams almost certainly didn’t work – or the person with a cure could claim $100 K
Have you written posts denouncing scammers or set up a $100K fund to give people some markers about what might work and what certainly doesn’t?
Carping is cheap. It also underestimates the ability of readers out there to sort the wheat from the chaff. Every day I get inputs from people out there picking up on aspects of these posts feeding back ideas that tell me things that I didn’t know.
Ordinary folk have worked out there are major problems with the antibody tests. No-one is certain that the biopsies are going to offer anything much. The only way we are going to know for sure is getting tests done and see if patterns emerge.
If you’ve anything substantial to contribute on p 63, ACE2 or anything else, please send it in – we’ll run it as a post – but getting picky about a post that you claim you knew was not written to explain things in detail seems pedantic
D
Sturm says
I have to say, I am one of the hopeless. I’ve only had PSSD symptoms since early August, but I also developed akathisia a few weeks later after I discontinued Abilify (which I also only took for a few weeks previously). My life has been completely destroyed by psychiatry. The completely moronic psychiatrist, who ultimately is responsible for basically killing everything I ever was, initially even gave me Haldol, even though I am not schizophrenic or bipolar! I wish I knew better before all of this. I wish I could have discovered this site before all of this happened.
If I was ever suicidal in the past (and I was), just imagine how bad it is now. I’ve witnessed everything I was completely disappear into the abyss. I’ve lost it all.
It is especially difficult for me, considering I have Asperger’s Syndrome and tend to become beyond fixated on certain subjects. I have been put through a lot of pain in my life, but nothing comes close to any of this. I just want it to end.
I hope that, if reincarnation is real, maybe I’ll be given a better shot next time. Or maybe parallel universes indeed exist, and I will be able to experience an alternate version of myself, who never had to go through any of this. In any case, I just cannot do this anymore.
I wish I was treated like a human being, but instead I had my rights violated by charlatans, who violated the hippocratic oath, and I am the one who has to suffer immensely whilst they get to continue on hurting more innocent people.
H.C says
Dear Dr.Healy,
I am not saying that it is easy to communicate about PSSD. Many people are in a desperate situation. Unfortunately, as you have denounced in previous articles, some people try to take advantage of it. I am aware that you have to take these things into consideration when you write an article.
You are by far the person who has done the most for our cause (EMA recognition, research initiative…) and I am grateful to you. I did not write my comments with the intention of being gratuitously critical or picky. I just noticed that some people had misinterpreted your article and it seemed to me that some points added confusion. It was just my impression, I may be wrong.
Sincerely
Dr. David Healy says
H
Sorry if I’ve been too hard on you. Of course there are people trying all sorts of things. They are as desperate as I would be in their situation and I might well be among those who reach for risky things. No-one can stop this or even say its wrong. The only way to keep people safe is to work on finding a cure and holding out some hope that there might be something better and safer than what they (or I) might be about to try.
With a problem as desperate as this, no one is going to be happy with what is happening. RxISK got given out to for setting up a RxISK Prize – we were told we should put the money into reeaarch. Now that we are putting money into research we get given out to or have people demanding to know what potential treatments we see on the horizon.
The way to save people from making mistakes are not notes of caution but investigating p63, ACE2 and some of the other proteins mentioned on the Research Forum page – chasing researchers who may have the answer to our problem but just they don’t know about the problem. I would feel a lot happier if even 1 in 10 of the folk with PSSD who have been in touch with us put some effort into contacting researchers and raising the profile of the condition and the need for input.
I personally am more confident about what Luisa Guerrini is doing that any other research happening, both confident in the work and in her, but this is still just one promising angle and solving a problem like PSSD needs lots of promising angles.
I am also confident in the skills of the PSSD community to come up with good ideas – too many people figure they are not researchers and cannot make a contribution when in fact they can.
D
Jacob says
Since i had Covid i’ve had circulation issues, sexual dysfunction and general anhedonia. Now been 9 months.
I can say that before this my gut microbiome would almost certainly have been in dysbiosis due to many rounds of antibiotics, also potentially mercury toxicity from my fillings.
The only time i feel like i get a window is sometimes during fasting – and heavy meals certainly make it worse. I lean towards the idea of gut issues triggered – most likely leaky gut. I think the gut has a huge role to play across the spectrum. And like with PSSD, long covid also affects ACE2 receptors, which happen to be abundant in the gut.
My brother suffers with full blown PSSD and this research is very promising. As he has heart issues from the PSSD and possibly lymes, he has does have access to ACE Inhibitors but has never tried them.
I’ve read that ACE Inhibitors can upregulate ACE2 receptors which is promising, i’ve suggested he trial the meds and see if they make a difference.
I’ll be sure to let you know anything i find.
Jacob
Dr. David Healy says
This comment came in from someone with PSSD and a dermatological condition
I thought I’d give you an update regarding my genital itch. I finally got to see a dermatologist after over a year’s wait by taking a last minute cancellation.
The dermatologist does NOT think I have lichen sclerosus, which is good news. (I understand why it would be unwise to include someone with LS, an autoimmune condition, in a trial designed to test for SFN which may also be due to autoimmunity.) She attributed my complaint to dermatitis. I asked her whether it could be due to PSSD. She admitted that she had looked up PSSD while I was getting dressed and said that anything that causes vaginal dryness could cause chronic itching. My appointment was on the day the ‘A Cure for PSSD, PFS and Post-Isotretinoin Syndrome’ appeared on the Rxisk blog. Having read it on the way to the appointment, I asked her if the itch could be due to SFN. She said that it was possible too.
I then told her about the stuff on p63 and ACE2 and that as a dermatologist she should be interested. Her ears pricked up. I told her that it could provide a common mechanism between PSSD, PFS and post-isotretinoin syndrome. “You know how isotretinoin can cause permanent sexual dysfunction?” “Erm, I have heard of that.” It was quite interesting to me that she was willing to look up PSSD and didn’t rule it out as a cause of my problems, yet became very guarded when I raised isotretinoin causing a similar thing… Drs are quite good at pointing out problems in other specialisms but aren’t so good at self-reflection.
I told her that I may be called for an SFN trial and that I would let her know the result. “Once the mechanism is known, you can better inform your patients if this risk!” She looked a bit sheepish and I left.
Klaus says
Dear David,
in case that Prof. Guerrini is not aware, please point out clearly to her that PSSD is so much more than “just” a sexual impairement.
Those of us who are affected severely know that this is just the tip of the iceberg and that emotional blunting and cognitive impairment can fool not only the most beautiful triviality in the world but almost every fundamental aspect of life like work, sleep, social interaction, … (could be a looong list here)
Thus in my opinion any scientific research about PSSD should primarily focus on the severe cases in order to find a solution for the most badly injured of us. If you argue that the sexual dysfunction is the most prominent PSSD-symptom and thus an appropriate candidate for a starting point, i fully agree. But PLEASE take care that research about PSSD does not only focus on the sexual aspects but also takes the wide range of other severe and sometimes life-disabling symptoms into consideration.
Thanks for your work and for holding out hope…
Klaus
Sarah Browne says
What type of cells were these assays performed upon?
Dr. David Healy says
The human immortalized keratinocytes HaCat cell line was maintained in DMEM medium enriched with 10% fetal bovine serum, L-glutamine 1mM (Euroclone), 100 units/mL penicillin and 100 μg/mL streptomycin (Euroclone).
Arjan says
The key finding of this study was a decreased gene expression of ACE2 in patients with ME/CFS compared to healthy controls, which could mean a could be at a higher risk of developing severe symptoms of COVID-19.
https://meassociation.org.uk/2021/09/research-summary-are-people-with-me-cfs-at-higher-risk-of-complications-from-covid-infection/
Biggiebigpoppa says
Dear Dr David
I have a question about SFN. Can people have weaker blood flow during SFN, which leads to cold hands, feet and because of this people can have a little restriction of movement in the joints (e.g. wrist)?
Dr. David Healy says
Blood flow and nerves go together – as blood flow falls, nerves die. Can be hard to tell then exactly what is causing the cold hands and feet
D
Arjan says
Is it known if the neurons also die or if blood flow issues causes axonal damage only?
Since the following study showed the ability to regrow CNS nerves(optic nerves in this case) in after introducing 3 genetic factors (a subset of Yamanaka factors)
This study was done on mice https://www.nature.com/articles/s41586-020-2975-4
They are currently trialing monkeys, and would go on with human trials in 2023 if the non-human trials go as expected.
Boost says
Hello Dr Healy
I would like to remind you again.
That myself suffering with pssd and many others where caused by ashwaganda ksm66. There are people taking powder and sensoril , but the vast majority of cases are from ksm66.
Some after 2 weeks and most after 4 weeks of exposure, some just a few days. I took just 300mg, half a tablet which caused myne started hyperthyroidism, derealisation immediately which lasted 2 months and hyperthyroidism (something stuck in the throat sensation almost gone after 3 months)
My tsh t3 t4 is fine, cortisol, adrenaline. Yet I can’t feel adrenaline or my heart beating (barely)
I had stroke like symptoms on the first 3 days. There are many people becoming anhedonic and losing emotions from ashwaganda ksm66. Which lead to a lot of people thinking is was a heavy metal toxicity, or mycotoxins.
I think it’s important to do comparisons, and potentially will be able to provide a mechanism.
There are many reports spread across the internet for ashwaganda pssd. In my group of 100 people affected by ssri, snri, antipsychotic, accutane, finasteride, there are 14 members with ksm66 pssd.
This is where a lot of people thought of the 5-ht1a desensitisation because of ashwaganda mechanism directing 5-ht1a to 5-ht2a. People have been suffering for years with ashwaganda pssd, with matching(identical) symptoms.
https://www.ergogenic.health/blog/ashwagandha-can-cause-anhedonia-pssd-blunted-emotions-and-apathy
He has been suffering for 7 years and hasn’t recovered.
Myself like many others suffering with pssd, have also experienced tinnitus induced by my pssd, myne is in my left ear and seems to affect a lot of other pssd sufferers on the left side. Many others with ashwaganda pssd also experience tinnitus on the left side.
Ashwaganda ksm66 pssd symptoms, anhedonia, no emotions, numbness over whole body, genital numbness, ED, pleasureless orgasm, no brain gut connection or brain genital connection. Tinnitus, lost the sense of temperature, taste. Derealisation, depersonalisation (loss of ego, sense of self). Inability to feel supplements, caffeine, smokes, alcohol etc can’t feel hunger properly or when to go to the toilet. Loss of pain sensation, not able to feel the atmosphere, inability to feel energy or feel tired. Mostly just fatigued all the time, brain fog. No warm cozy feeling, no oxytocin, social withdrawal, ( feeling nothing when you hug someone ) not waking up feeling refreshed. 24/7 ground hog day, some people have visual snow. Suicidal ideation.
There are a lot mechanism of withanolides. I just feel this is important because it’s also used regarding cancer, which may affect not only the immune system but the p53 family and p63, p73, prok2 and PROKR2. Also a good gene marker the lab told me to do is ENDO1 and ENDO2 to find mismatched DNA, mutations and cell death.
Hopefully this can provide some hope that if a supplement can cause this and produce the same symptoms it’s traceable and we will be able to compare withanolides mechanism with ssri for a diagnostic marker.
Kind regards
Boost909
Sandman says
Hello Dr Healy
More discussions have come up regarding antibiotics and the functions GLT-1 and the affect antibiotics has. We have seen cases cured by taking antibiotics, amoxicillin, flagyl etc
(Not in that order and it would appear flagyl seems interesting)
Just wondering how these affect gut microbiome, we have had people taking candibactin, berberine and seen alleviation in symptoms. Someone with a course of 3 months no has no symptoms apart from low labido and numbness.
Nicotine self-administration session. This synaptic potentiation was associated with an increase in both AMPA (GluA1) and NMDA (GluN2A and GluN2B) receptor subunits, and a reduction in the glutamate transporter-1 (GLT-1).
Since we don’t feel the affects of nicotine and GLT-1 has been looked into for the treatment of addiction, and is affected by antibiotics I’m curious, as it also affects nmda.
What we are lacking in our group of 100 members is methylation tests. Microbiome seem to either be fine or some have h pylori or candida. Although a lot have high streptococcus. Some have no candida and still have pssd but have other bacterial strains on there panels. Some with insanely highly RANTES on there cytokine panels while having undectable amounts of cytokines. Organic acids seem fine, although inconclusive some others are finding mycotoxins. Some people’s akkermansia where low on microbiome.
After looking through papers on gut microbiome and secretion I found the following neurotransmitters.
Lactobacillus acetylcholine gaba
Bifidobacterium gaba
Escherichia norepinephrine 5-HT and dopamine
Streptococcus and enterococcus 5-HT
Bacillius norepinephrine dopamine
I would also like to bring up a particular case where someone was cured with Neo40, aside from its other ingredients which can be obtained the thing that makes it Neo40 is sodium nitrate.
https://alisonvickery.com.au/online-shop/product/neo40-professional/
I can’t find reference to the dose, with sodium nitrate being dangerous, but affecting the patients nitric oxide production iNos Nnos etc I find it interesting, in your medical opinion is sodium nitrate safe to consume. ( we are talking about specifically the period of time for treatment advised by the product manufacturer and not intended for any other use )
Notes from paper:
The sodium-dependent glutamate transporter GLT-1 (EAAT2, SLC1A2) has been well-described as an important regulator of extracellular glutamate homeostasis in the central nervous system (CNS), a function that is performed mainly through its presence on astrocytes. There is, however, increasing evidence for the expression of GLT-1 in CNS cells other than astrocytes and in functional roles that are mediated by mechanisms downstream of glutamate uptake. In this context, GLT-1 expression has been reported for both neurons and oligodendrocytes (OLGs), and neuronal presynaptic presence of GLT-1 has been implicated in the regulation of glutamate uptake, gene expression, and mitochondrial function.
Uncertain of sodium nitrates affects on GLT-1 and how it affects the expression. This is just more information.
Kind regards
Boost909
Jacob Cook says
I previously mentioned about my brother’s severe case of PSSD. I’ve done a lot of research into PSSD and personally believe it stems out of gut dysbiosis. He has just had a full microbiome report back from Healthpath which indicates very strong gut dysbiosis.
All key butyrate-producing bacterias are very low (particular F. Prausnitzii), these are essential for preventing intestinal permeability (leaky gut). Gram-positive bacteria are very low overall (particularly Firmicutes).
Levels of gram-negative bacteria are very high (particularly Bacteroidetes)
Furthermore if you go on the PSSD subreddit you and search for gut reports, you will not find a single report of someone without gut dysbiosis.
ACE2 is expressed heavily in the gut and i think lots of research needs to be dedicated to this area as a potential source of the problem. SSRIs have been proven to affect efflux pumps and other parts of the gut that could potentially induce dysbiosis, as well as acting as an antimicrobial.
Thank you for all your efforts and i hope we can cure this truly evil condition.
Jacob
Walther says
Gut Dysbiosis is likewise commonly implicated in various autoimmune diseases, like coeliac disease and IBS. It could be that it isn’t the root cause, but rather a symptom. I’d be interested to see how often people with Long Covid test positive for it.
Jacob Cook says
I personally have long covid and yes i do have gut dysbiosis, much research has proven that gut dysbiosis is present in long covid and is a key marker
In terms of the gut and PSSD, i’ve seen many cases now of people recovering from PSSD by addressing their gut issues – most commonly SIBO, SIFO, strong dysbiosis or a combination of the three.
This would suggest at least in those PSSD cases that the gut is the source of the issue and not the symptom.
Reddit-user says
Hi fellow sufferers. The New York Times ist looking for people suffering PSSD to write an article about it. This could help us all. So if you fit the criteria, please get in touch!
See:
https://www.reddit.com/r/PSSD/comments/10b2cu4/ny_times_journalist_is_interested_in_writing_a/
Sam says
I believe we should focus on the numbness of the genitals in all studies. Other purported symptoms such as emotional blunted and cognitive impairments are difficult to measure. The numbness aspect is highly measurable with nerve tests.
Matt says
Dr. Healy- first of all, THANK YOU for your tireless work to help all pssd sufferers. You are a hero to all of us! Second, I came across this article about a potential breakthrough in treatment. Just wondering if you had any thoughts on this? https://pubmed.ncbi.nlm.nih.gov/36135826/#:~:text=PSSD%20is%20a%20rare%20clinical,no%20effective%20treatment%20is%20available
Mike says
Vortioxitine gave me PSSD I now have sexual dysfunction for over 3 years after taking it. Many articles claim Vortioxitine is safe but that is not true and there are many other PSSD sufferers saying that Vortioxitine caused their PSSD also. I have been on many antidepressants and Vortioxitine is the only one that gave me sexual dysfunction I am now stuck with PSSD because of this drug.
Dr. David Healy says
At RxISK, we agree vortioxetine can cause PSSD and has just the same effects on p63 and ACE2 as other SSRIs.
DH
Matt says
Thank you, Dr. Healy. This is why I have such confidence in RxISK, because your team is focused on finding a true cure for PSSD. Something about that study didn’t seem right. I plan to donate money to RxISK for PSSD research, I know it will be used well!
andreas says
Hey sandman, (and others)
I read some of your comments and I ask you to read some of mine. They are written down in the forum: https://rxisk.org/forum/epigenetics/ => andreas says… (2 comments)
I think we have to ask three questions to the drug of SSRI:
First: what are you doing, what is your aim?
Answer: I want to extend the duration of action of the endogenous serotonin by raising the endogenous serotonin-level in the synaptic gap.
Second: how do you do this? How is your mode of action?
Answer: stop the reuptake (only) of the endogenous serotonin from the synaptic gap into the presynapse thus the endogenous serotonin can remain in the synaptic gap.
Because of that I am called a selective serotonin reuptake inhibitor. (SSRI)
Third: Every drug needs one single target for market approval. What is yours?
Answer: my target is the gene SLC6a4.
Because if you switch off this gene (by dna-methylation with the help of CH3-groups which i do have in my chemical formula) there is no more production of the serotonin transporter SERT (5-HTT) and this enzyme/protein is responsible for resuming the endogenous serotonin from the synaptic gap into the presynapse. Without that enzyme SERT, the endogenous serotonin remains in the synaptic gap and that extends the duration of action of the endogenous serotonin.
My personal opinion: the SSRI switches off gene SLC6a4 with the help of its CH3-groups (DNA methylation, like all Inhibitors just like isotretinoin, finasteride, etc) and thereby prevents the production of SERT (serotonintransporter; 5-HTT). This SERT transports the endogenous serotonin back in the presynapse and ends the long-lasting presence of endogenous serotonin in the synaptic gap and the acting on the serotonin receptors.
This should be the fundamental background for all research.
This is the key, because all of these horrific side-effects/unwanted-effects are caused by too much endogenous serotonin acting.
Switch off gene SLC6a4 => No SERT => too much and long-lasting endogenous serotonin acting in the body with following side-effects/unwanted effects. (ALL have the same cause/basis)
The SSRI itself does not act directly on the serotonin receptors in the brain or in other parts of the human body. It is passive, like most of the drugs in the market.
SSRIs only stop the production of the SERT.
The SSRI only ensures the non-reuptake of endogenous serotonin.
Then too much endogenous serotonin act on the serotonin receptors in the brain and in other parts of the body.
Maybe the body of SSRI sufferers can not break down (demethylation) these CH3-groups and the gene SLC6a4 is permanently switched off.
=> permanent no SERT => permanent side effects/unwanted effects.
Maybe you have to test the methylation pattern of the gene SLC6a4 and the amount of the product of the gene SLC6a4, the SERT. (serotonin transporter; 5-HTT)
Stop the permanent non-reuptake of endogenous serotonin from the synaptic gap into the presynapse and you can stop the permanent side-effects/unwanted effects.
Only the permanent absence of SERT and the following permanent, long-lasting acting of too much endogenous serotonin in the synaptic gap and the serotonin receptors is the reason for these horrific side-effects/unwanted effects, so I am thinking.
Every single of all these horrific side effects/unwanted effects could be related with too much acting of the endogenous enzyme/protein serotonin. You could read about it everywhere.
My key side-effects/unwanted effects are my insomnia, restlessness and PSSD (genital numbness) which started immediately by taking pill number one. The only one.
This drug has to be the reason for all these horrific side-effects/unwanted-effects. From this moment I became another person.
Also all the other side effects/unwanted effects are influenced by the endogenous serotonin level, all side-effects/unwanted effects have the same background.
If you solve one you solve all.
I think that it “only” needs “one pill” (maybe CRISPRon/off) with the endogenous substance, SSRI sufferers do not have, which resolves the CH3-groups from the gene SLC6a4, it would be switched on again and we get our lives back.
It must be the absence of an endogenous substance because most of the people taking these drugs (SSRI, isotretinoin, finasteride) do not have permanent side-effects/unwanted-effects, that means their body can resolve these CH3-groups.
The mode of action of the SSRIs is much less complicated than we all think.
We have to think “kis”. (keep it simple)
The SERT (serotonin transporter/5-HTT), the product of the gene SLC6a4 must be produced again.
Imagine, if this theory is right, solving this problem would be very cheap, fast and almost easy. It is worth trying it, right?
Best regards
andreas
Callum says
Thank you Andrea. The PSSD community and rxisk.org need people like you. This sounds very promising to me, the naked eye. Whatever happened to us on the medication was not damage, was not neurotoxic activity. Something was modified and that modification persists. Almost all of us can say that. This sounds perfect to me. Let me know if there’s anything I can help with pushing this theory forward.
Andreas&C says
Dear Dr. Healy,
my wife and I want to support you on your journey to find the reason behind PSSD. And maybe her Story is helpful to you/your research:
My wife (32 years old) was never depressed. She got an SSRI (escitalopram) as a treatment of sleeplessness and anxiety. None of us was googling any symptoms or side effects in advance.
She took in total 3 pills in 6 days (0.5 pills/day). As we had a very active sex-life and she also enjoyed masturbation a lot, she was recognizing a change very fast after the pill on the 3rd day.
She was feeling numb and was not able to reach orgasm. As it was not possible the other days, too, she decided quickly to stop taking escitalopram after the 6th day.
In the first week after, the focus was on the sexual impact of the pill but during the day she recognized that she was not getting any good feeling anymore. In the past she was very very sensitive, empathic and enthusiastic – in general a very kind person to everyone. But on this day, she was not able to laugh, love, or just enjoy anything. The days before she was also not, but was focused on the sexual issues. So it was not recognized. That was the second she started googling side effects and found also your research.
It’s been more than 3 months since, and these days have been absolute hell for her – I don’t have to tell you the details, I guess. Basically, the same as for most who do not feel anything anytime anymore (not just sexual).
Based on the article “A cure for PSSD” I also did some research (I’m an engineer and pretty logical person) and read not only your articles, but all explanations to every vocab in the paper I was not familiar with. I came to the function of the renin-angiotensin system / renin-angiotensin-aldosterone-system (RAS or RAAS). And I just hope that the following (very obvious) anomaly of my wife is useful for you and your research:
My wife never was “normal” in respect of sweating and her skin moisture: She used to have VERY dry skin, with a lot of loose (dead) skin every day on the whole body. It was much worse in winter as in summer and it was so bad, that you could peel of the skin everyday at nearly every point of the body. Not even special cremes from pharmacy were helping against this.
Also, she was not sweating at all. Literally NOT. If she was doing workouts, sex etc., she got a very red face/head, but her skin was dry as a desert. In summer/in the sun: no sweat at all on the body. She was forced to go to the bathroom very often, as the water consumed was not sweat out. This was just reduced to sweat. Her vulva was normally wet at any time.
Since escitalopram this change 180 degrees she has the smoothest skin. No loose skin at all. Not even a little anywhere on the body. Also is she sweating “normal” in all possible situations (during sport/under a blanket etc.). And she does not have to go to the bathroom as often as before. Her vulva was extremely (dripping) wet in the first 4-6 weeks after the SSRI. This has changed back to normal again.
So we hope these crumbs are helpful somehow, as this is an extreme obvious change on her body.
What is she doing at the moment? We hope that some “gut theory” is correct, and she is supplementing bifidobacteria infantis at the moment as it is one of the few things which do at least no harm. Also, she has a loving family with her and we try to stay as positive as possible.
A question at the end: Did you see any connection in your research so far for the duration of the side effects and the time/amount of taking the medicine?
Thanks for your work and for your engagement!
Whishing all the best to all of you!
Boost says
Hello Dr Healy
I currently run a discord server for pssd.
We are currently trialing my theory.
I have seen 100% remission of first trial.
Although it was messy and has a lot of other measures.
Hoping next trials to be more accurate.
Will continue to update you.
More trials to continue over the next weeks to see if this is noteworthy.
I would rather not discuss my theory at this stage.
I have researched the mechanism heavily. Just putting the puzzle together.
Do you have a more private avenue of discussion ?
Or contact email.
Kind regards
Boost
Malu says
Hey Andreas!
How is your wife doing now?
I was exactly like your wife, very emotional, sensitive, very empathetic and hypersexual.
Now I feel like a stone, since 1,5 years. This is a nightmare beyond words.
How is your wife doing by now?
I would be happy to get an update and possibly some hope…as I am at my end.
Best wishes,
Malu (female, 27)
Callum says
Stay with us Malu. I am feeling near my end too but we need to keep moving, and advancing the research. Epigenetic and gene silencing theory is very promising.
Best of luck.
menx says
hello dr healy,
i know this sounds crazy perhaps but i drank camel urine temporarily and after it erection hardness 100% out of 0% i feel like i found the cure but for some reason i did not get reply back on my mail. (sorry for bad english), i have no idea why camel urine did that. after stopping camel urine i do not experience erection anymore maybe 5%. maybe this is an individual thing and it only worked for me or it might work for others? please dr healy dont ignore this i swear i saw improvements.
my email cenkhan321@outlook.com
meen_28x
Boost says
Hello Dr Healy
I’m like like to share my theory as reference for potential cure.
We will have further trials starting around 25th to 6feb.
To keep it brief.
Regarding the master switch PGE2, EP1,2,3,4.
Immunoglobulins therapy.
Bovine serum albumin.
Kind regards
Boost
Martin says
Good morning .
I would like to share my story. In January 2020, I started taking Parogen, at a target dose of 60mg. The compulsions after this drug disappeared, but I made a terrible mistake and in November 2020, I suddenly stopped taking this drug. What happened to me then is indescribable. Nightmare fears, total insomnia, intestinal obstruction, heart problems. Trips to the emergency room, calling an ambulance home.
From insomnia, I thought I would collapse and die. I couldn’t sleep, neither during the day nor at night.
I am now a wreck of a man with ruined health. I have clogged intestines, problems with breathing, heart, lack of strength and condition, blood vessels in my eyes have broken and they do not heal despite a long time since stopping the drug, my receptors in the brain are destroyed. I still got drug-induced anhedonia, I’m sitting lifeless, I don’t feel literally anything, my drive has decreased and I’ve lost my former vigor. I have a void in my head, despite my extensive knowledge, I can no longer talk about many topics as before.
I paid a high price for my stupidity in suddenly stopping Paroxetine.
I want to warn everyone not to make my mistake.
Michal says
Is rhACE2, SAE0064, MLN-4760 a potential treatment?
Dr. David Healy says
Good question. We don’t know enough to predict. The only way to know is to try. Meanwhile we need all the reports we can get from folk on ACE inhibitors (ACE-1) or Sartans also called ARBs. Do these help or make things worse.
David
Stefano says
Hello Dr. Healy,
I have been taking Tremfya (guselkumab), a biological drug, for years to treat my psoriasis. Can this affect the pssd?
Dr. David Healy says
I dont know
D
jrod says
Hi Dr. Healy,
Has Dr. Guerrini performed these same assays with p53 and/or MDM2?
There is some research to suggest p53 is a rallying point in the treatment of acne including the function of retinoids
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5606086/
Additionally the AR, which is often implicated as a key point in these conditions, is likely reflexive/codependent of p53 expression
https://pubmed.ncbi.nlm.nih.gov/18084622/
https://pubmed.ncbi.nlm.nih.gov/22859066/
I recently spoke to a fellow PFS sufferer who experienced a full recovery he attributes to the use of PGE2, a substance often used out of scope for hair loss. Researching this further I stumbled across research that PGE2 can impede apoptotic and cell arrest signaling induced by p53 as a result of ionizing radiation damage.. potentially paralleling the cell cycle arrest and apoptosis you note Dr. Guerrini has observed here
https://pubmed.ncbi.nlm.nih.gov/32735825/
I plan on testing this compound myself and will report again here if we find anything noteworthy.
Thank you for your continuing work in fighting these conditions.
Nikolas says
Promising! But people get PSSD from Doxycycline too including my self. I hope whatever cure they find will be available for us who had Doxycycline.
Dr. David Healy says
Its an SSRI – so the answer is probably yes
D
susanne says
Unsure where to add this so will pop it in here
3 of 5
Publication of the report of the expert safety review of suspected psychiatric and sexual side effects to isotretinoin
MHRA Unsubscribe
1:51 PM (7 hours ago)
Report of the Isotretinoin expert safety review is published
View as a webpage / Share
MHRA_Banner
The report of the safety review of suspected psychiatric and sexual side effects to isotretinoin, conducted by the Isotretinoin Expert Working Group and the Commission on Human Medicines (CHM) is now published on GOV.UK.
For more information on the outcomes of the review see our News story.
The Isotretinoin page on GOV.UK has been updated and includes links to:
The report of the CHM Isotretinoin Expert Working Group and a plain language summary of the recommendations
Recordings of the patient and stakeholder meetings in July 2021 for those who gave consent for these to be published
Recording of the public CHM meeting that considered the review
Minutes of the CHM meeting on 17 December 2021 when CHM made their recommendations on the review
The MHRA is working with patients and other stakeholders including clinical organisations to finalise the implementation of the recommendations of the expert review. The CHM has formed the implementation advisory group to advise on how best to introduce the new measures into clinical practice.
No new action is currently needed from patients and healthcare professionals while the process for implementing these recommendations is being finalised. There will be further communications about implementation following completion of the process.
If you have any further questions, please email info@mhra.gov.uk.
Kind Regards,
Patient, Public and Stakeholder Engagement team
Genevieve says
Have you considered the effect of Thymosin alpha 1? It acts on ACE2 enzymatic activity.
I know someone who had severe myocarditis after a covid vaccine. Steriods left them bed riden, Thymosin a1 helped them recover.
Here is a study on its effect on covid patients: https://pubmed.ncbi.nlm.nih.gov/35226991
Could this agent be useful to consider?
Matt says
Dr Healy- you have written in past articles that perhaps the key to unlocking pssd and its mechanisms lies in compiling a database of all meds that cause sexual dysfunction and finding the common ground (i.e. maybe like an enormous excel doc?). On that note, what about using the recent AI/chat gpt technologies? I have read that they have used these technologies to analyze the stats of the greatest athletes of the 20th century (and stocks, etc) and the computer has found patterns that human researchers have not previously noticed. While I do not think computers are ready yet to diagnose patients, I think there is great potential that one of these programs could use existing knowledge of these meds and their chemical contents and perhaps identify the mysterious needle in the haystack.
Dr. David Healy says
Matt
If you or someone else wants to do this – fine. Am not at the moment impressed with the ability of ChatGPT to help in this area. Some people have been asking it questions and the answers are unimaginative – so far
The problem for ChatGPT in this area is it can only go by searching all drug labels for instance = but companies don’t enter data like this in the labels. If you could get it to search all internet forums that might be interesting – but you need to ask more than sexual issues – you would really need to be specific about things like numbness.
David
David
Erik Hermanson says
I have heard that isotretinoin causes apoptosis in the Leydig cells. I have been tested for testosterone levels around 300pcg/dl which is normal for a 70 to 80 year old man. I am wondering has there been a mechanism or biological feedback loop that has been identified that has been compromised as a result of isotretinoin? Do we know why testosterone levels decrease so drastically? I have found that fish oil pills with omega three’s cause some improvement in libido but I am very frustrated that I will have permanently low testosterone as a result of this medication and that there is no going back for the rest of my life. There are people on forums online that are desperate to recover but have wild theories about what has been altered epigenetically and have strange ways of experimenting about what could possibly set them back to normal. I am hoping there is a way for the body to go back to normal even if that means the return of acne. However looking at how fetuses and then babies become deformed from isotretinoin, there appears to be no way for the body to go back to normal. There is certainly no cure for the deformities that fetuses experience so it doesn’t seem likely that there is a cure for the changes that happen from isotretinoin.
A.M-B says
Hello Dr. Healy,
Since you wrote “We are awaiting results of a clinical trial currently in progress to see if a trial in PSSD makes sense.” I am wondering, how is the clinical trial going? Do you have any feedback so far? And will there be a trial for PSSD?
I find the theory of ACE2 and it’s effects on the RAAS (and therefore on many other things in the body) very interesting. It somehow relates to some different success-stories which people described in the past.
(For example following
> Hormon-Treatment success-stories (RAAS is affecting this obviously)
> Taurin Success-stories (Blood pressure affected)
> Cardamomin success-stories (effects on Blood pressure as well)
> Differnent Sport success-stories (also obviously affecting blood pressure and hormones))
AndreasM says
Basic question here: What is meant by “ACE2 Receptor”? Is it the same as “Angiotensin-II Receptor”.
I don’t find any clue what the enzyme 2-receptor shall be…?
From my understanding:
ACE2 is the enzyme that fullfills the task of producing Angiotensin II which fullfills the task of enlarge tissue. While the Angiotensin-II Receptor is the target-place where Angiotensin II (not ACE2) will be activated.
Q: Is the enzyme (ACE2) blocked in its production or is the receptor (Angiotensin-II receptor) blocked?
The pictures say ACE2 is vanishing, but the text implies that some receptor is damaged…
Will Rob says
Dr Healy,
Important to note that there have been 3 reported cases of men in their mid to late 20s who took finasteride that committed suicide and that when an autopsy was conducted showed atrophy of the hippocampus.
Dr. David Healy says
no
Genevieve says
This is a very interesting article by a cardiologist on long covid treatments:
Refer to http://www.ncbi.nlm.nih.gov/pmc/articles/PMC9520195/
Summary: “we here propagate a multidimensional approach targeting major regulating pathways involved namely the RAS-bradykinin axis, the cholesterol metabolism, and finally the intestinal microbiome. In detail, AT1RB (angiotensin II type 1 receptor antagonist/blockade) rebalances the RAS-bradykinin-axis, statin-therapy improves endothelial function and elicits pleiotropic anti-inflammatory effects all together stimulating immunomodulatory pathways. These two drug therapies should be governed by a histamine-reduced diet limiting mast-cell effects, reducing inflammation, and potentially restoring the intestine microbiome.”
Malu says
Hey Dr. Healy!
We already have been in touch via Email.
You wrote “We are awaiting results of a clinical trial currently in progress to see if a trial in PSSD makes sense.” I am wondering, how is the clinical trial going? Are there any results so far?
And which “old” drug are you talking about? Would a trial for PSSD make sense?
I look forward to hear from you.
All the best,
Malu
Mark says
Dr Healy, I have emailed with you quite a bit. I am the one that had some sort of full reversal for a month of all pssd symptoms, brain fog, sexual dysfunction, and even full sensation came back in genitals. This was where I was put on wellebutrin after getting pssd. I didn’t think it was helping initially and even was maybe making me slightly worse. So I was told to taper off. The only way to taper off since it’s a coated pill was to go to eod. When I did this on the day I had to take a dose I still had pssd and on the off day I’d have some sort of rebound where I was 100%. Better. This continued until I stopped and I was better for a full month then woke up one morning again to having all the symptoms again. Does any of this tie into ace2 receptors? Is there any studies on wellebutrin and ace2? Could it do something to change these receptors that quickly?
Dr. David Healy says
M
I have no idea if there are links. But when we think we have an answer it should be able to explain things like this. Events like yours indicate the problem is not permanent damage.
D
WaitingforResurrection says
To test autoimmune hypotesis, is it possible to give autoimmune treatment in animal study after giving SSRI? Is it even possible in animal study?
PSSD dont happen for everyone, so is it possible that people who have tendency get autoimmune disease will have it?
Raffard says
Ashwagandha causing PFS/PSSD is reported absolutely everywhere, including in the very first messages of this thread. Celebrity doctors such as andrologist Cameron Maximus have been raising the alarm (several posts of his twitter account). Denmark has banned it as of spring 2023, based on a 2020 Denmark Tech University study, and activated a EU mechanism alert, in order to seize stocks abroad destinated to Denmark. Sweden and Finland are following, Poland and France already have reacted. The ashwagandha infamous bubble is about to burst.
Simple question : why doesn’t ashwagandha appear on the RXISK database (or does it?), and why excellent doctor David Healy doesn’t write a small piece about it?
Ashwagandha’s destroying lives. It’s causing full-fldged PFS/PSSD, and very severe cases, after very short exposures : testemonies are everywhere. I’m one of them. Victims are facing invariable distrust from their doctors and even their lawyers.
A small contribution from fine polemist Dr David Healy could have a really heavy impact on the receptivity of the subject by tribunals. Brands need to be prosecuted and contribute to the research, such as Milan University’s Dr C. Melcangi and Tampere-Kiel’s Drs Urbanucci and Hornig (that seem to be continuing Baylor Colege’s findings).
Getting PFS/PSSD from a short exposure to a seemingly innocent supplement is an infamy going beyond imagination. It is dystopian.