: 
This is a tricky talk. ADHD and Autism Spectrum Disorder (ASD) are not simple medical disorders. They come with a lot of baggage.
There is a video version of the talk here with the slides and text and links to related articles or posts below. You can make all slides below bigger by Clicking on them.
Slide 1: The Report you see above, issued at the end of May, is 444 pages and is the first of two telling the UK it’s in big trouble – it’s about to lose a generation with ADHD and ASD playing a big role in this. The catch-phrase is Britain is paying 25 times more on benefits for young people out of work than it’s paying on efforts to get work for them.
A week after the talk was recorded, a guy called Healey Britain’s Defence Secretary, semi-stating the country can grapple with ADHD/ASD or with Putin but not both, resigned, triggering an attack of serious political vapors,
Slide 2: A 1980 medical document UK politicians know little about – DSM III – lies at the heart of this crisis. Faced with a divide in US mental health between Freud on one side and new psychotropic drugs on the other, in an attempt to get people on the same page, DSM introduced operational criteria. These center on things we can observe and agree on – like poor sleep, loss of energy, suicidality etc – unlike neurosis or neurotransmitters which are ideas not observables. Both sides can agree that if you have at least 5 of these 9 observables you can be diagnosed as depressed.
In 1980, DSM also said a doctor must make a judgement call. You could have 5 features of depression because you’re pregnant or have influenza – your doctor must decide which it is. People harmed by meds know that leaving the decision to doctors doesn’t always work out.
In 1987, DSM quietly dropped doctors from being judges to just another juror. The same set of features could now be used to say we were both pregnant and depressed. And a door was opened to each of us deciding whether we were depressed or had ADHD or both regardless of what our doctor thinks.
This can’t be right either. We and whoever else might have a say in our diagnoses need to come to a consensus. We can’t just be told we don’t have ADHD.
Slide 3: Here’s another hot political potato. The Netherlands leads the way in diagnosing ADHD and ASD and in permitting euthanasia for mental disorders. A monitoring committee, in their 2024 report, outlined the case of an 18-year old with ASD who sought and was granted euthanasia. No evidence was offered that he had neurodevelopmental delay in childhood. He may have just recently been diagnosed. The relevant processes were followed and the euthanasia went ahead on the basis that ASD is supposedly incurable.
Slide 4: Zygmunt Bauman in this wonderful book told us the Holocaust is a window on our future not a painting of our past. Bauman claimed Max Weber had foreseen the Holocaust in 1920 when he said that once we had the technologies to do things, there would be pressure to do them.
In the 1940s before the Nazis exterminated Jews and other minorities, they began with children and people with mental disabilities – with lives not worth living. Horror-struck by this now, we forget that German doctors were then the most sophisticated in the world and the Nazis were very public health aware – they banned tobacco.
Their aim was to make their gene pool as good as it could be. The Swedes and others were doing this as well. 360,000 Germans were sterilized and 170,000 terminated.
In 1920, it was too early for Weber to spot that one of the most rapidly developing technology was what we now call marketing or propaganda or fashion. The goal of propaganda is to become invisible – to become fashionable.
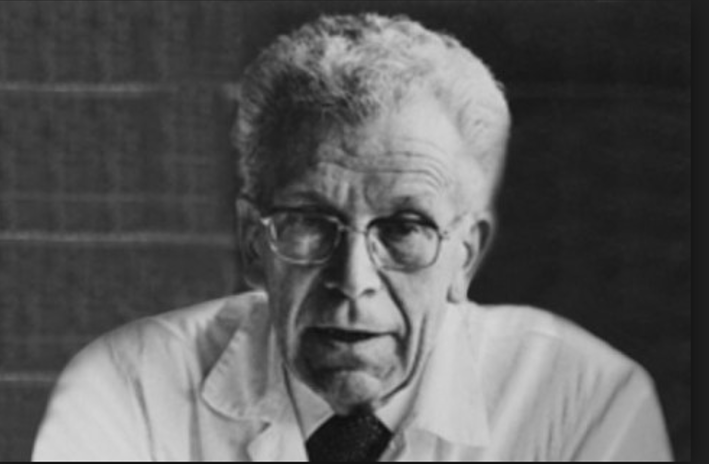
Slide 5: Here’s a friendly looking Hans Asperger, who back in the 1930s created Asperger Syndrome an early version of ASD. A mild mental handicap. A lot of these children got exterminated . Many parents were happy the decision was taken out of their hands.
Slide 6: In 1980, real people were grappling with real patients. Samizdat hosts 100 Interviews with many of these like child psychiatrists Judy Rapaport and Rachel Klein and some of the key folk responsible for operational criteria Bob Spitzer, Sam Guze and Mandell Cohen.
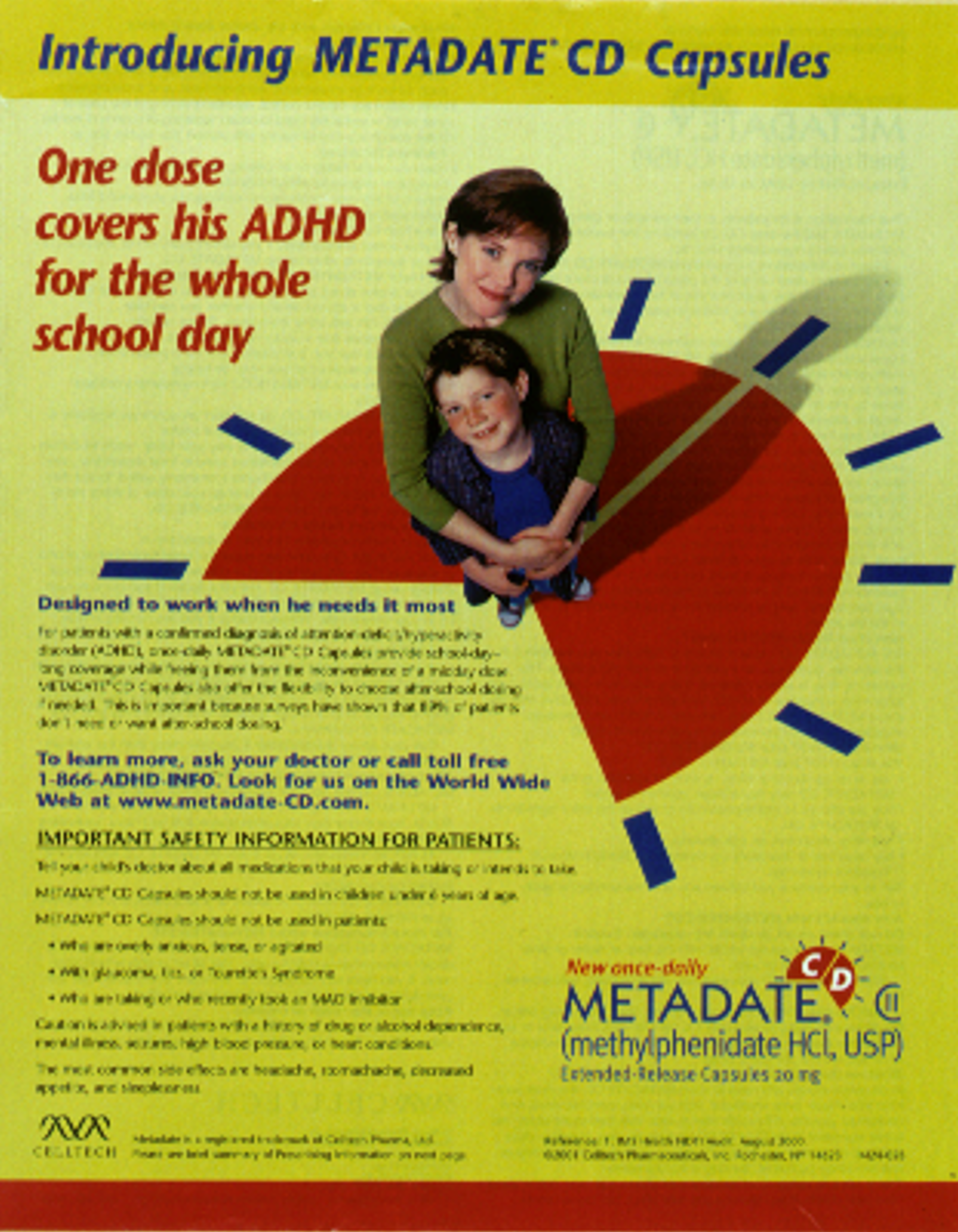
Slide 7: DSM III created the first ADHD criteria. Up till then, US child psychiatry had been a therapy bastion. They didn’t give drugs to children. Long before they began giving antidepressants or mood-stabilizers to children, the use of stimulants for children with ADHD broke the drug taboo. Drugs like methylphenidate and dexamphetamine had been around for decades and were off patent – but industry rapidly geared up to patent isomers and extended release versions of these old drugs aimed at profiting from this new market.
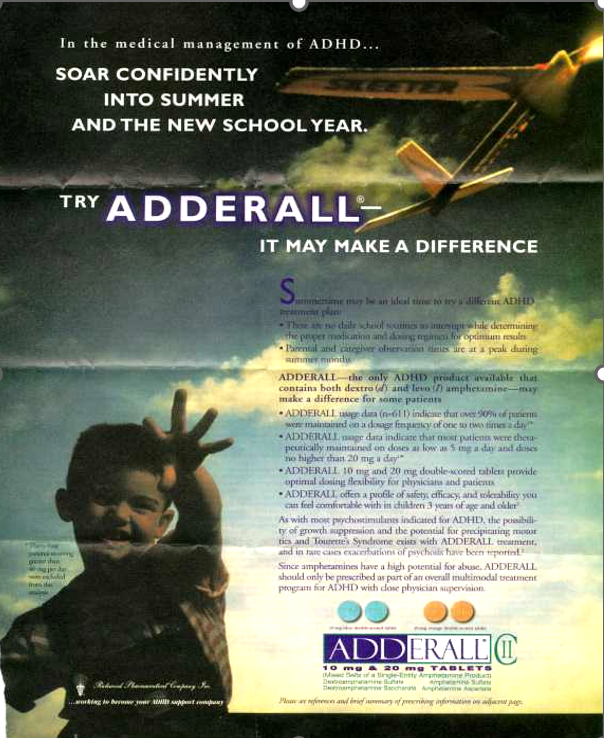
Slide 8: In addition to clones of Ritalin, dexamphetamine led to Adderall. Vyvanse and other expensive off-shoots.
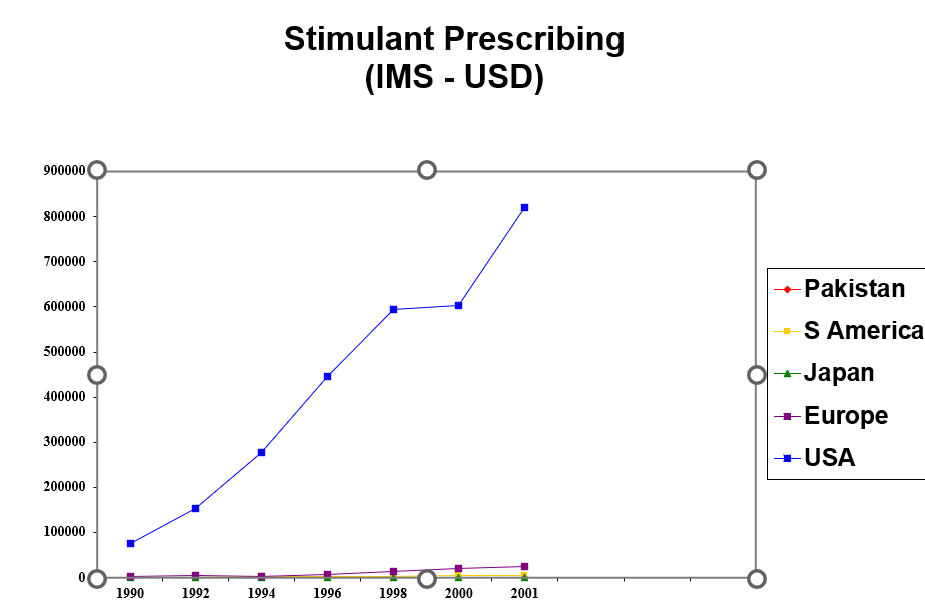
Slide 9: Stimulant prescribing and profits rose dramatically in the US compared to anywhere else. Giving controlled drugs to children became a compelling prospect for US medicine – which had replaced Germany as the most sophisticated in the world.
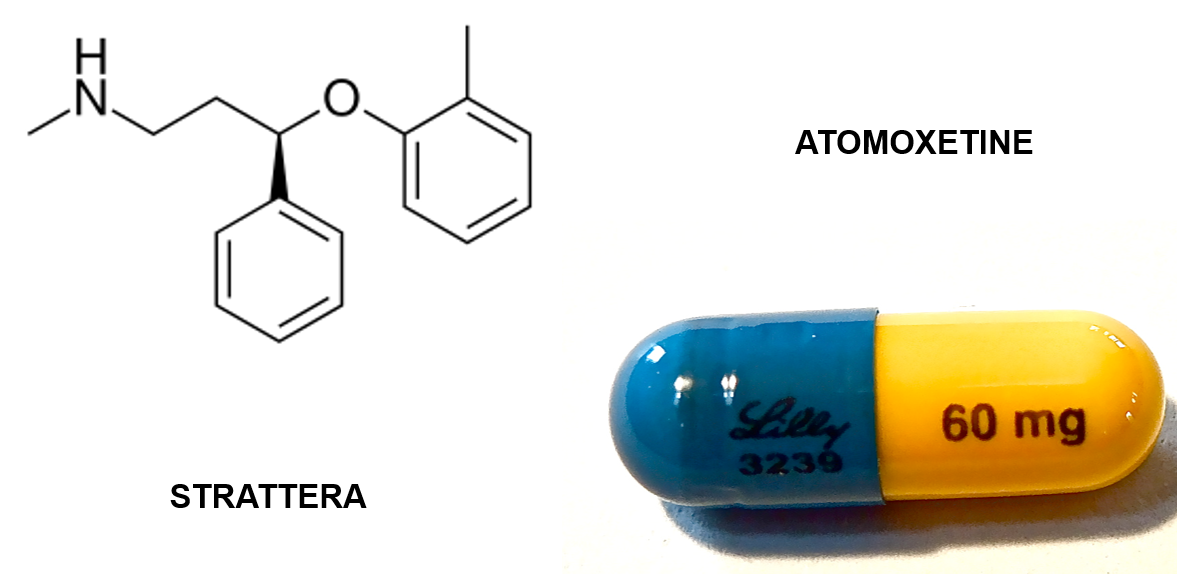
Slide 10: This Oxetine is the next step in the story. What’s an Oxetine? Fluoxetine Prozac is one. Nisoxetine – a noradrenaline reuptake inhibitor was the first. When Lilly decided SSRIs were a better bet, a bunch of Oxetines like atomoxetine were left behind. Until John Heiligenstein suggested maybe they might help with adult ADHD.
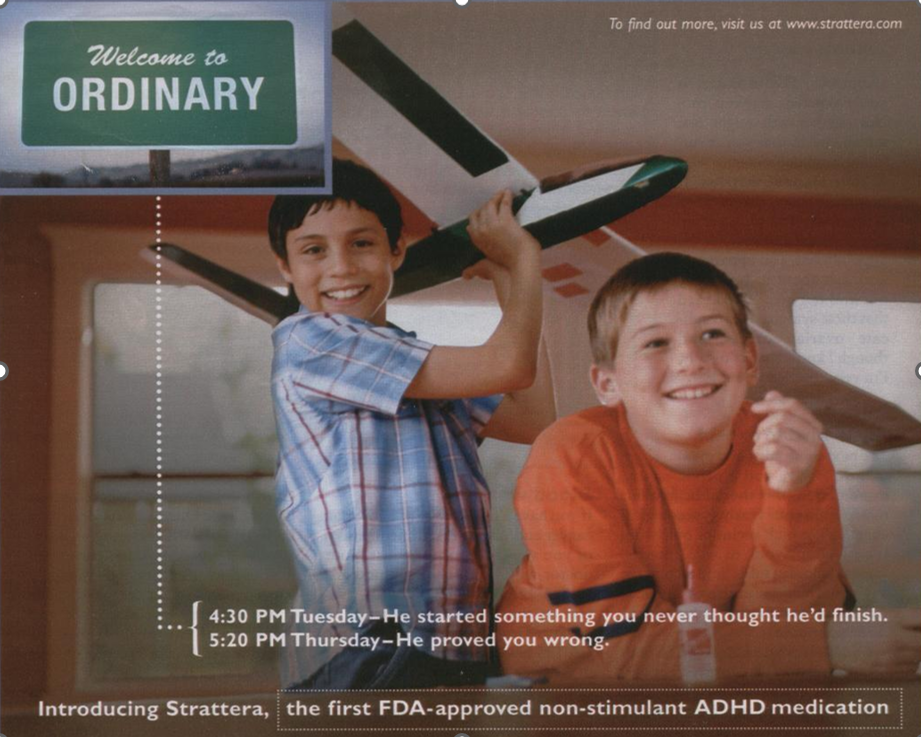
Slide 11: Atomoxetine, branded as Strattera, was brought on the market as you see here – as safe for ADHD because it was not a controlled drug.

Slide 12: In 1992, adult ADHD was beginning to take off in America – Driven to Distraction was the Listening to Prozac of the ADHD market. Kids don’t grow out of ADHD it told us and it’s not just boys who have it – girl’s do too – more attention based than hyperactivity based.
Slide 13: By the mid to late 1990s, the US was deep into a full scale transition from a Freudian Psychobabble to a Psychotropic Biobabble.
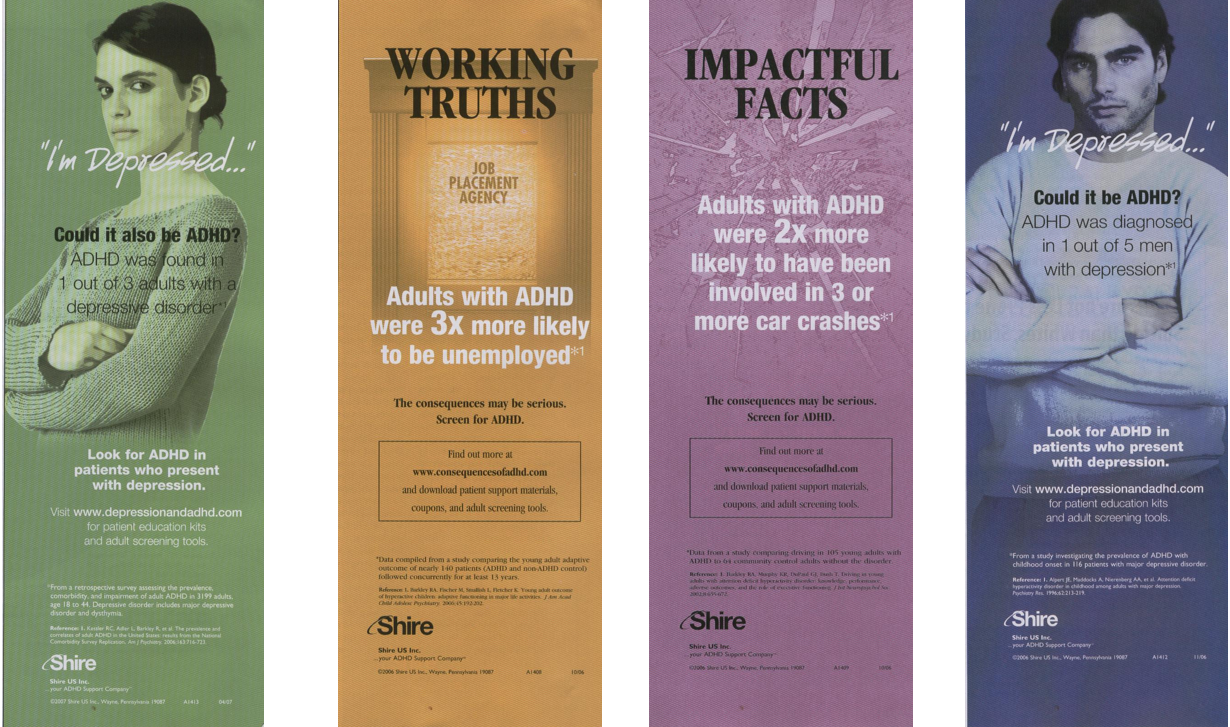
Slide 14: Adults were now seeing adverts for the consequences of not treating their ADHD – failed marriages and careers, accidents, suicides. And of course you no longer had to give up depression to get ADHD – you could have both. You could add ADHD meds to your antidepressants. Atomoxetine did a great deal to create this new market
Slide 15: Around 1997, it was almost impossible to give a stimulant to a boy with ADHD in the UK. This British Association of Psychopharmacology meeting brought child psychiatrists and regulators from the US, Europe and the UK along with pro-therapy psychologists. The aim was a Consensus Statement – getting both sides of a divide to find common ground.
An agreement that no treatment works for everyone made it possible to switch treatments to see for instance if a stimulant helped when therapy hadn’t and vice versa.
A consensus, however, is a flimsy defense against the most powerful disseminator of modern fashions – the pharmaceutical industry.
Two of the people at the meeting were authors on the then unpublished Study 329.
Slide 16: In 1943, Leo Kanner introduced a new illness – Autism. A condition caused by frigid mothering, affecting 1 in 10,000 children.

Slide 17: As the prevalence of autism increased, a range of factors like drugs taken in pregnancy and genes began to come into the frame. Heavy metals like lead and mercury were invoked. Vaccines, which gave a distinctive story – my child was fine up till about 15 months when he had a vaccine and immediately lost skills he’d had up till then, were fingered partly because they contained a mercury preservative.

Slide 18: Autism Spectrum Disorder didn’t appear until the 1990s. As more and more of us were being recognized as having oddities, it made sense to incorporate Asperger’s Syndrome into Autism as a mild form of the problem and Lorna Wing was the main person who proposed this.
The prevalence of Autism Spectrum Disorders rose from 1 in 10,000 to 1 per 1000 and now stands around 1 in 40. Uta Frith was another academic linked to the ASD idea who recently said when we get to prevalence figures like 1 in 40, something has gone badly wrong.
Slide 19: A 1959 book by James Wilson created Teratology – to investigate abnormalities in fetal development. A Teratology Society was established in 1960. In 1961, thalidomide turbo-charged this new science. Recognition grew that other drugs like Diethyl Stilbestrol (DES) caused vaginal cancers in daughters. Drugs active on serotonin systems were flagged as risky – of which Bendectin, a drug for morning sickness in pregnancy is one.
By 1982, the idea that altered behavior rather than gross birth defects might be a teratogenic consequence was accepted.
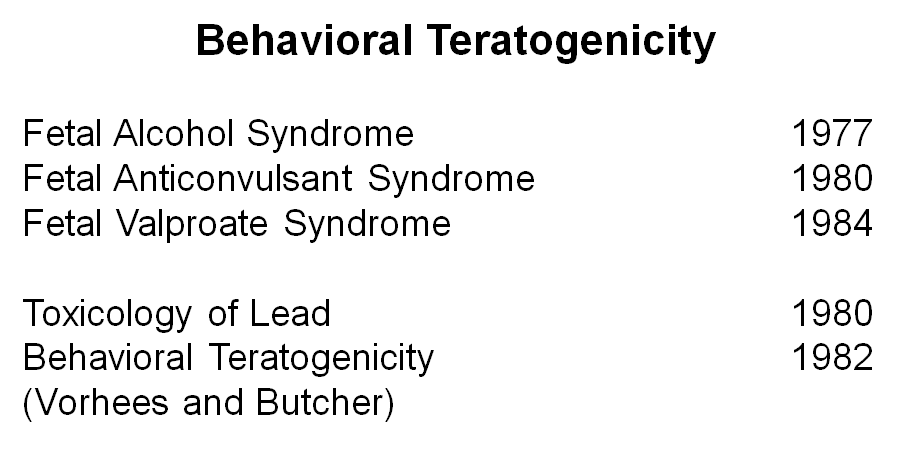
Slide 20: Recognition of the behavioral effects of drugs was driven by fetal alcohol syndrome and the effects of anticonvulsants, especially Valproate along with heavy metals like lead and mercury.
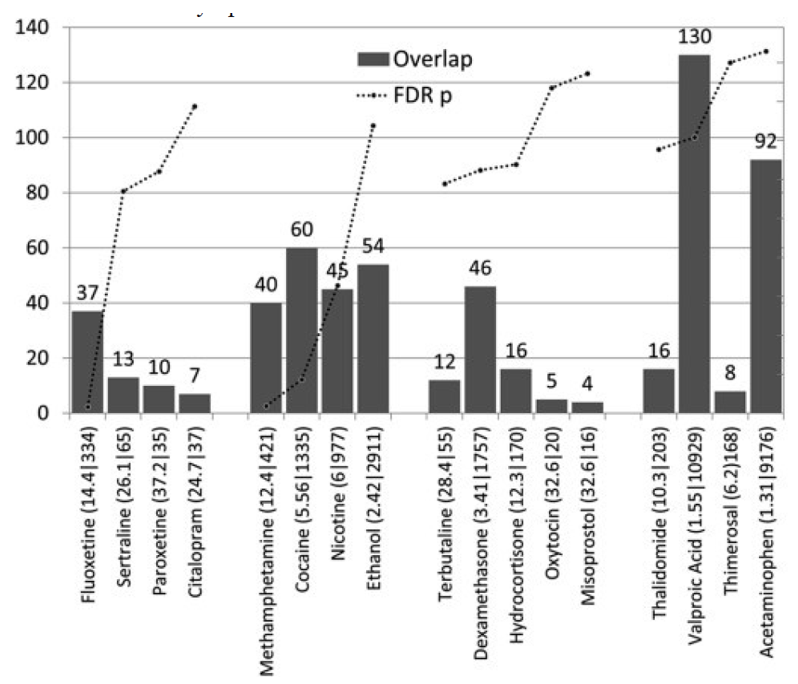
Slide 21: Teratology played a big part in the development of epigenetics. We learnt that medicines taken in pregnancy might turn genes on or off. Around 250 genes are risk factors for ASD. None of these cause ASD – but interacting with environmental factors they can lead to ASD.
Valproate is the standout column here – it interacts with something like 130 of these genes. Just to the right of Valproate is a tiny little column – that’s mercury, which had been the big concern. To the right of mercury is the next tricky looking drug – paracetamol – acetaminophen.
Anticonvulsants and SSRIs are problematic and paracetamol is both anticonvulsant and active on serotonin systems.

Slide 22: Now here’s an astonishing slide. From Thalidomide onwards there was a general sense that medicines should be avoided in pregnancy. FDA had categories for drugs A, B, C, D, and X. But this began changing. And many of the people who advised caution swung around to saying take more not less psychotropic drugs in pregnancy.
What is going on. From the early 2000s companies faced legal actions for SSRI caused birth defects. In 2009 GSK lost a Paroxetine birth defect case which ultimately cost them roughly $1 Billion. A lot of what you read now is aimed at minimizing risks – to companies, not mothers or infants.

Slide 23: This APA ACOG joint statement gives you an example of what happened. These professional bodies are saying even a minute you spend being miserable or anxious will harm your child. Take the meds.
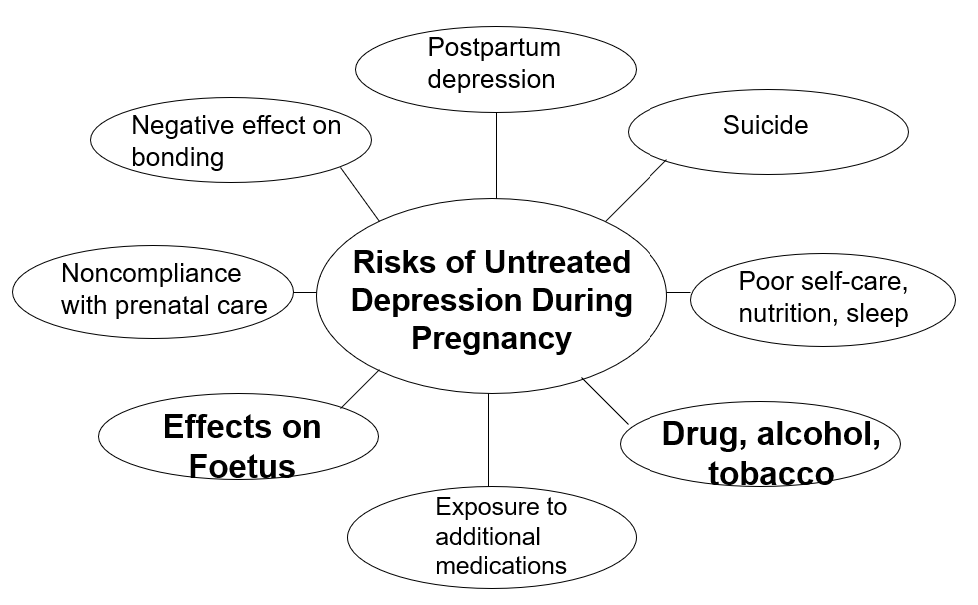
Slide 24: Tons of articles appeared with illustrations like this blaming untreated depression for causing things to go wrong. Untreated women will drink, smoke, and not eat. Poverty will cause them not to eat not depression. There is no evidence even severe melancholia causes birth defects. The idea that a woman’s mental state harms her unborn child is primitive medieval thinking.
Slide 25: This was happening not just in the most sophisticated medical country on earth – even in obscure offshore islands like the UK you got the same story as in this book written by well-respected people.
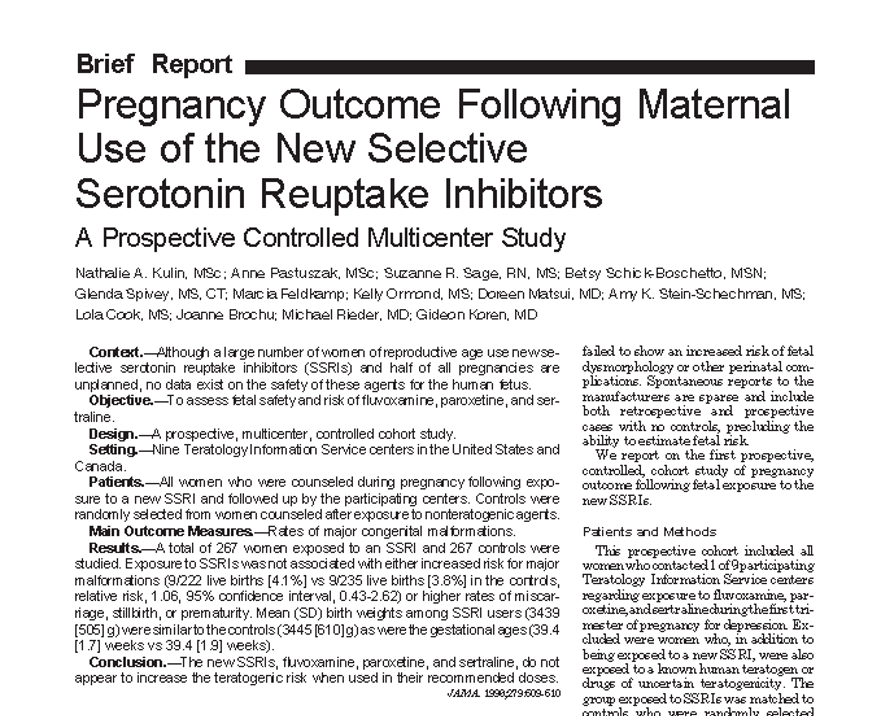
Slide 26: Canada’s now infamous Motherisk Group were quick to jump on the new bandwagon claiming SSRIs were completely safe even though the data in this paper shows increased risks of voluntary terminations and miscarriages. Gideon Koren, the dude behind Motherisk, was consulted by GSK’s lawyers in birth defect cases at this time. His articles are now getting withdrawn.
Slide 27: Koren pushed the boat out with a 2007 proposal to pregnancy stamp meds to overcome women’s irrational neuroses about meds.
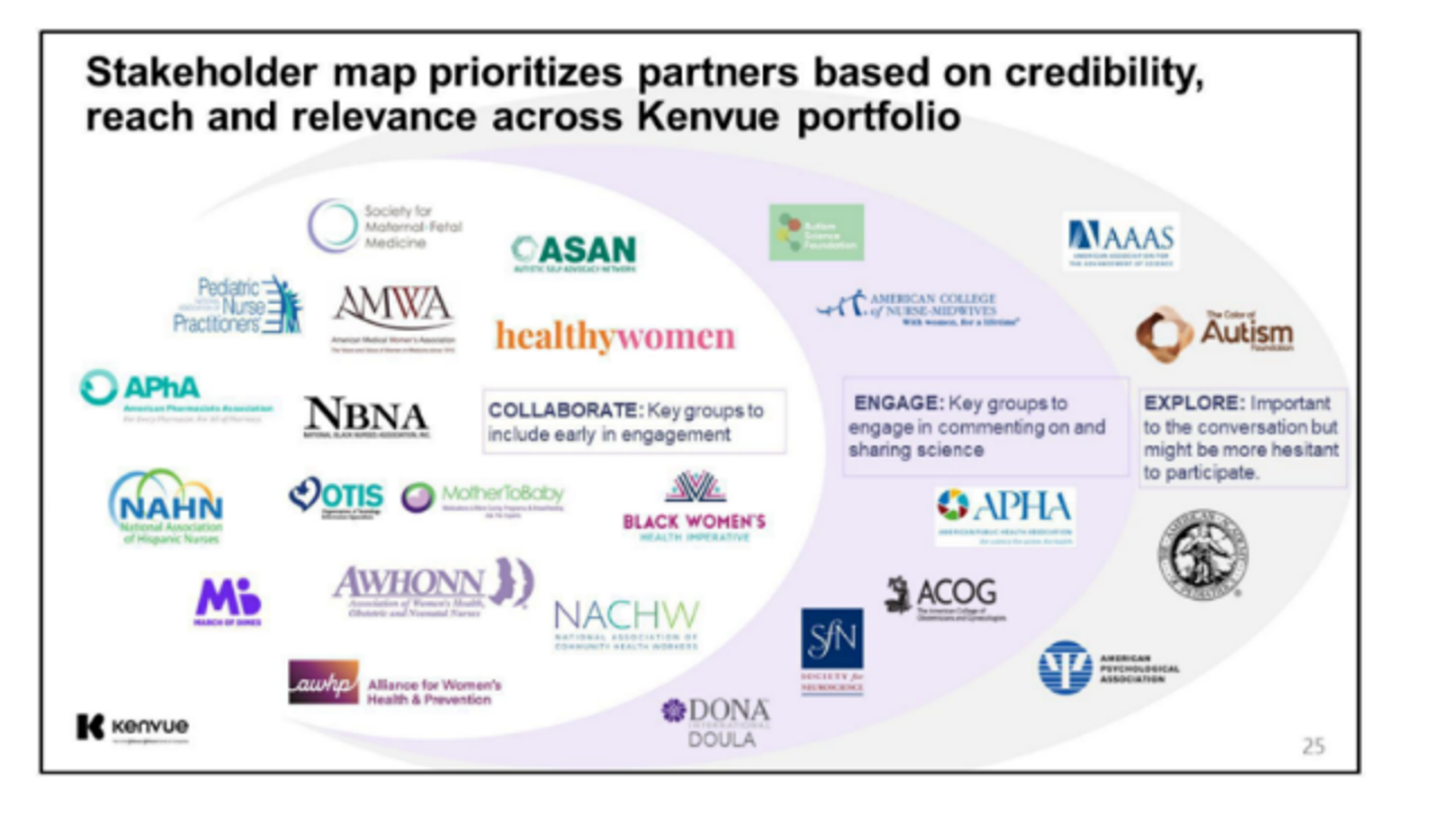
Slide 28: What you are seeing is the best propaganda money can buy – invisible behind the mask of science. Kenvue the name in the bottom left corner is Johnson and Johnson who sell acetaminophen – Tylenol – paracetamol. This slide was part of a Defend Tylenol program against evidence it causes ASD. Bodies like APA and ACOG feature as partners to J&J in their efforts to shape our thinking – See Partnerships in Healthcare and Unsafe Safety Systems and Tylenol and Autism.
Slide 29: Partnerships like this were evident back in 2004 when the APA were mobilized to resist Black Box Warnings on Antidepressants and wrote an embarrassing suicide note – saying We Believe Antidepressants Save Lives when they should have said Doctors Can Save Lives.
APA, AMA, ACOG etc are making it harder and harder for doctors to save lives now. Before showing you why, let me show you these two slides.
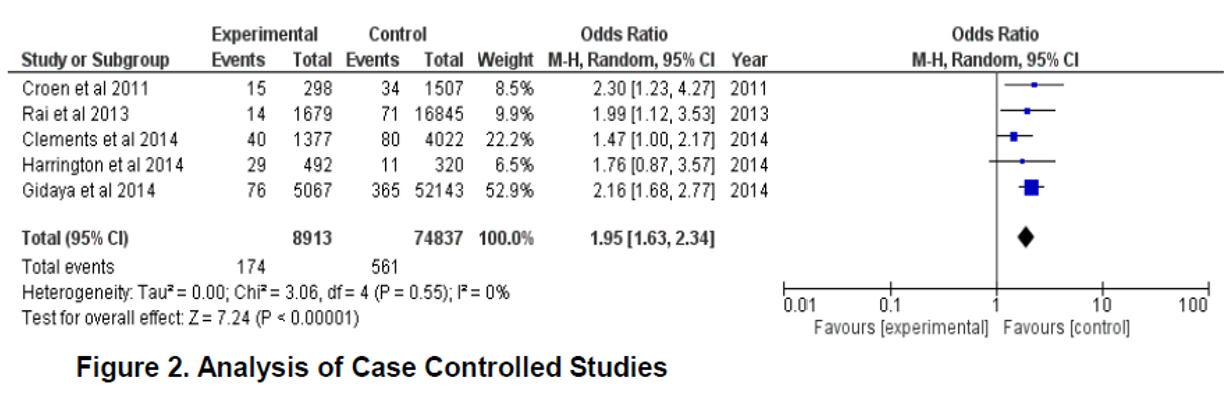
Slide 31: In 2009, GSK were found guilty of failing to warn about paroxetine’s birth defect hazards. As drugs that cause gross birth defects are linked to behavioral teratogenicity, a few of us figured we’d collect studies on SSRI links to ASD. These Case Control studies show a clear link. The article reporting this is SSRIs and ASD.
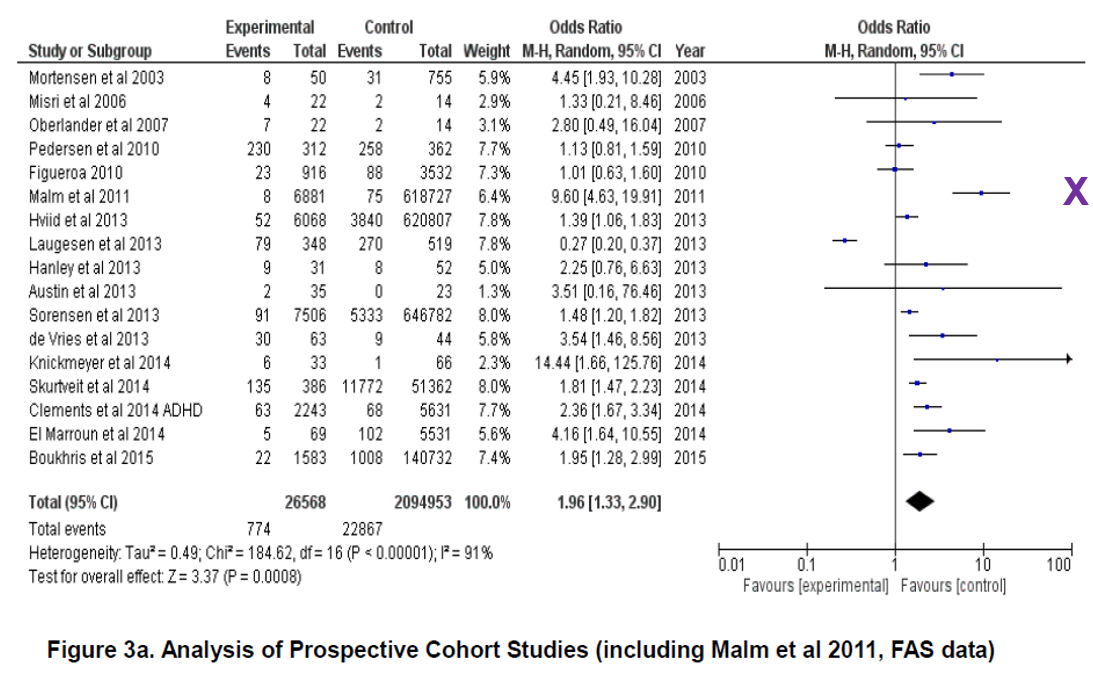
Slide 32: Cohort studies show the same result. The most interesting study is 6th from the top from Heidi Malm and colleagues, marked with an X. Malm’s results would have been even stronger had they not buried their most key finding in a footnote apparently because they couldn’t explain it.

Slide 33: In the Malm study there was a 10-fold increase in rates of Fetal Alcohol Syndrome Disorder in women taking SSRIs in pregnancy compared to women not on SSRIs. In an earlier slide you saw FASD being blamed on untreated depression – this is just not the case. The Canadian Guidelines for Alcohol Use Disorders now recommend stopping and not starting SSRIs.
Slide 34: We sent these very clear results to BMJ Open. The paper also included clear results from 7 animal studies showing neurodevelopmental delay – ASD – in the offspring of mothers taking SSRIs during pregnancy. You find a similar picture in both human and animal mothers given paracetamol/Tylenol in pregnancy.
Animals don’t do Fashions. It would be extraordinary if humans were the only animals not to show this effect. BMJ turned the paper down – saying we don’t publish studies with animal references in them.
Slide 35: Let me take you back to Britian in 2009, which still had no Adult ASD then. This back of an envelope study asked all 60 psychiatrists in N Wales if they figured there was such a thing as adult ADHD. None thought there was.
Asked what they’d think 5 years later – all but 2 figured they would think Adult ADHD was a real condition. Asked would they be treating it – half of them said yes.
This is one of the things about fashions – you can often see them coming.
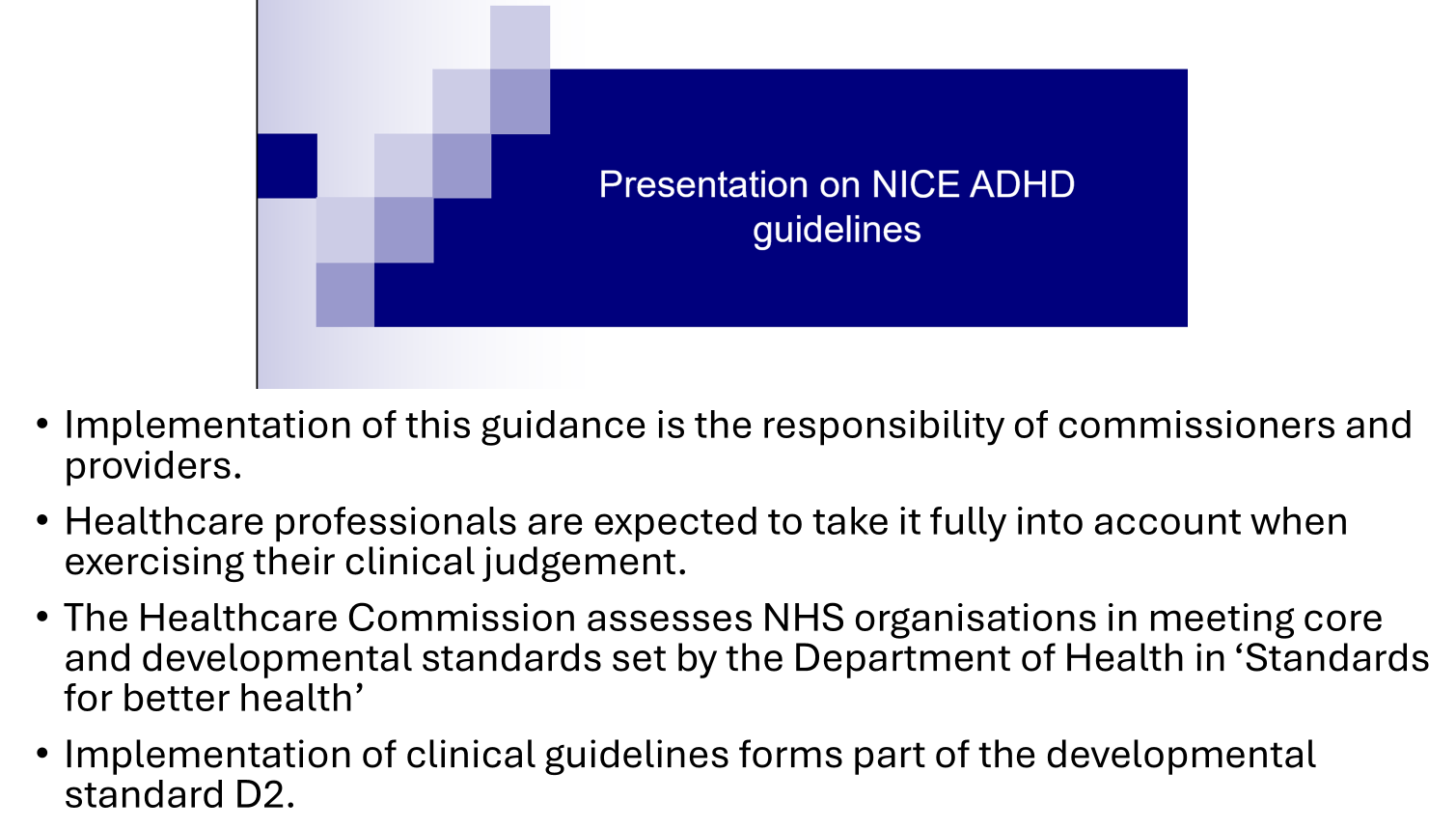
Slide 36: The initial NICE Guidance on ADHD followed the 1997 BAP approach – noting that it was a disorder of children and it was worth trying therapy first but be willing to switch to meds if no response. By 2018 NICE was telling clinicians in blunt terms Adult ADHD is real. Statements like the two below close to tell doctors they could be fired if they don’t recognize and treat adult ADHD – which means if the patient says they have it.
- Implementation of this guidance is the responsibility of commissioners and providers.
- Healthcare professionals are expected to take it fully into account when exercising their clinical judgement.
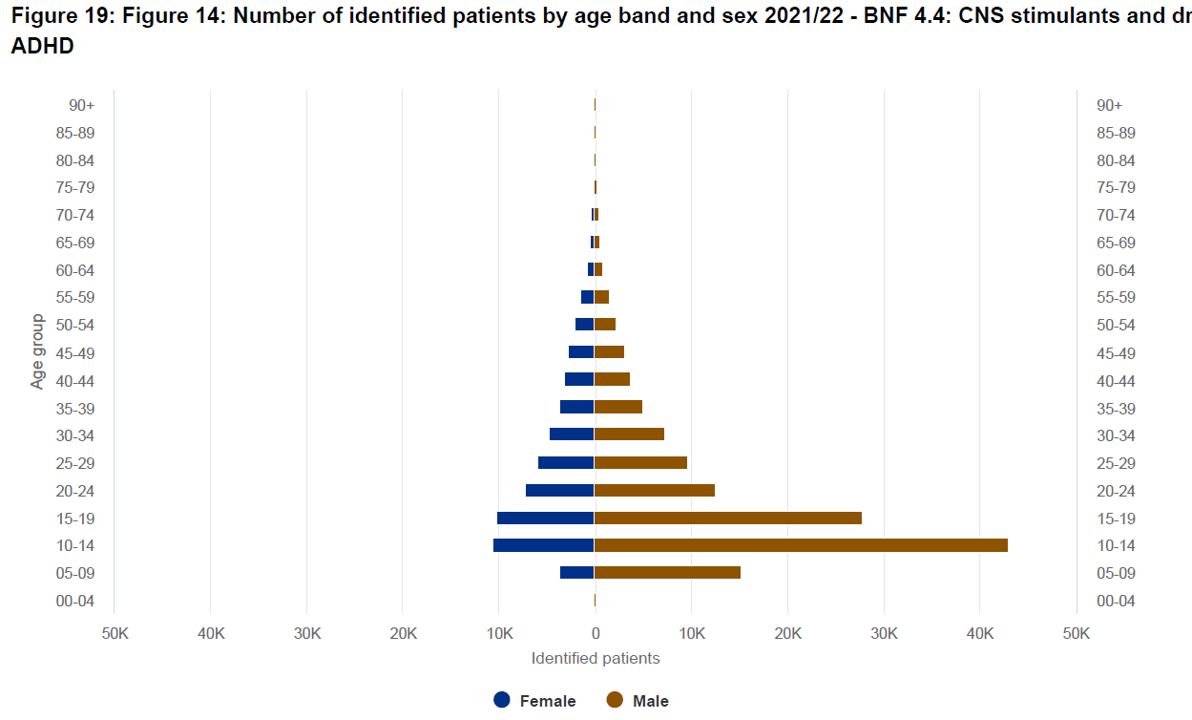
Slide 37: These 2021 UK data show you ADHD transforming from a condition of pre-teen boys to one on the cusp of becoming a disorder of post-teen women. Notice the tiny boxes up at the top for age brackets 60 to 90 – we’ll come back to this in the slide after next.
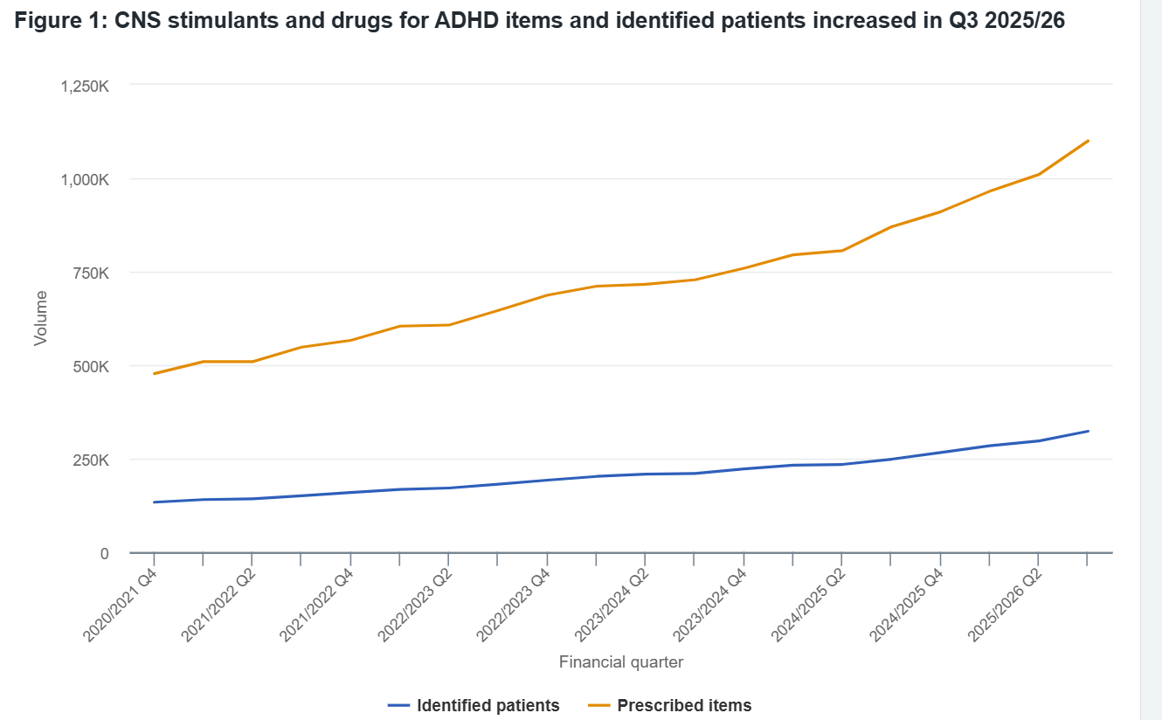
Slide 38: This slide gives you the 2026 figures for ADHD diagnoses and prescribing which doubles from 2021 to 2026. This is not because more children are being diagnosed – we have ever fewer children now. It’s adults, especially women.
Slide 39: The Carlat Reports were once viewed as a defense against pharmaceutical industry influence. Last month’s issues dealt with ADHD in old age and told us:
ADHD doesn’t disappear with age — its missed… obscured by cognitive complaints, comorbidities, and assumptions that attention problems are simply part of aging.
Demented patients used to wander endlessly from one end of a room to the other and back. Giving them a stimulant can stop this instantly – leaving them sitting down doing nothing. This is the opposite to what you might expect. It’s the same for hyperactive young boys who stop when given a stimulant. Even overactive manic patients stop. This response does not mean these people all have ADHD. It’s just an across the board action of stimulants on activity levels in motor systems.
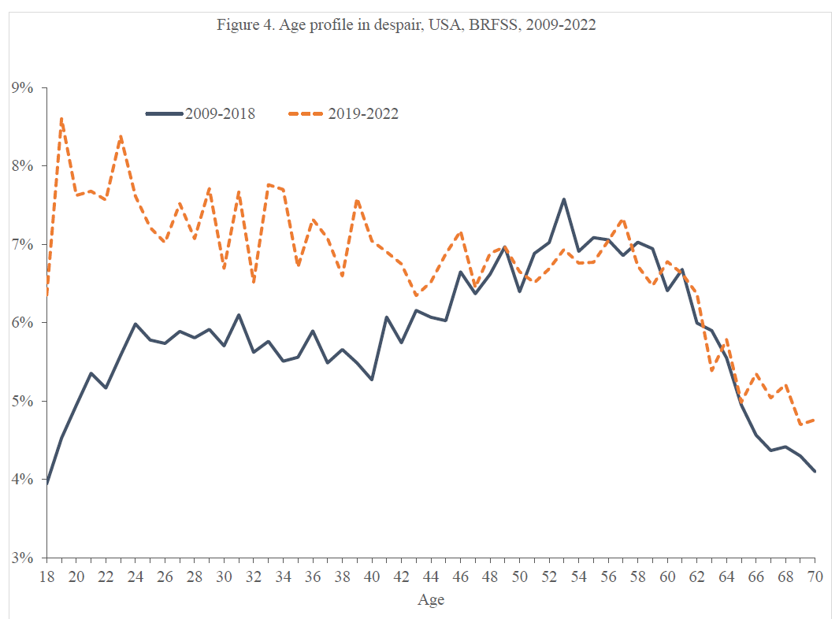
Slide 40: You’ve seen an increased spend on ADHD meds but this much bigger increase in spend is what is melting the British political system down.
The blue line shows what until recently was the most solid finding in all of the social sciences – claims for disability benefits peaked between the ages of 40 and 60 and were for Musculo-Skeletal problems.
As of 2019, this changes and the red line shows you the greatest collectors of disability benefits are between 18 to 35 for mental health reasons – primarily for ADHD, ASD and their comorbidities caused by polypharmacy that goes with treating all the conditions younger folk now have.
There are real disabilities here that do need benefit support but there’s something else. Every system can be exploited by smart folk. I’ve had university students who are in every social club in the university, who have a sense of humor when interviewed, who show no gaze avoidance talking to me – but when I suggest they may not have the ASD they tell me I’m an old dude who is not up with the latest research. They are and they know they have ASD.
Or another very bright woman at university tell me seriously she has 17 different conditions – and emailing me the list when I ask to see it. It contained both ADHD and ASD.
It’s not just smart university kids, it’s folk from well off smart families who have always been and will always be good at exploiting the system for themselves and their children.

Slide 41: All of this took another twist for Samizdat when we published Patrick Hahn’s Obedience Pills which gives a history of ADHD diagnoses in childhood in the US. This was way back before Covid. It seemed to make sense to reach out to the ADHD community and draw their attention to a book they might profoundly disagree with. They refused to engage. This refusal felt like the ‘you are transphobic’ message to anyone wanting to discuss what the Trans story tells us about Us.
This is not a jibe at people with ADHD – there is deeply worrying problem for all of Us here. We were sent a Video to show us the harms a hint of skepticism might do to ADHD folk.
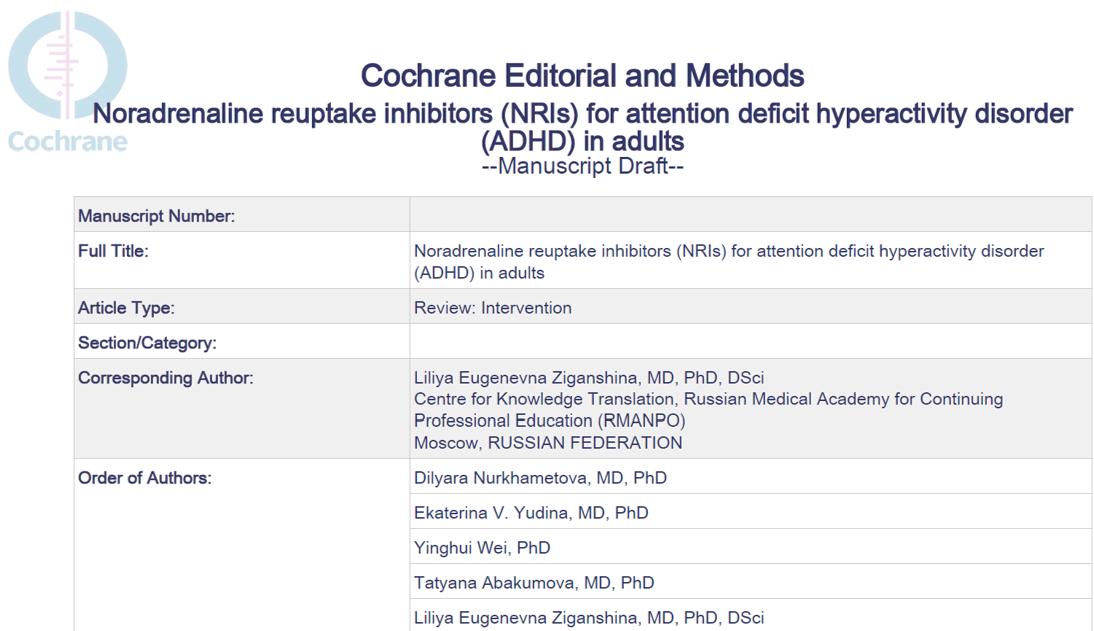
Slide 42: Even more than Carlat, for 30 years the Cochrane Collaboration was our defense against pharma. Recently Cochrane were presented with a review of the trials of atomoxetine for Adult ADHD. Atomoxetine is long off patent. Its trials were in the 00s. The review which looks like an excellent Cochrane Review was turned down for the following reasons.
Slide 43:
- The plain language summary mentions ADHD as “something that is thought to continue into adulthood” [this] could not only be insulting to the study population but is also not the expected wording for an academic article. It does not reflect current knowledge on the topic.
- ‘The omission of ASD as a frequent comorbidity is also a significant omission of the state of the art”.
This is bizarre. Cochrane Reviews cover RCTs and Lilly’s atomoxetine RCTs were only done for licensing purposes. In licensing trials companies do not include 2 indications. Back then, Lilly and others typically said adult ADHD is thought to continue into adulthood. The Cochrane authors echo Lilly.
In the 00s, Adult ASD didn’t exist. The outside reviewers Cochrane asked to vet the proposed Cochrane Review ran Adult ADHD/ASD clinics.
It is hard to resist the impression Cochrane has either gone Mad or is scared of a Trans-like backlash or upsetting some of its Industry ‘partners’. It doesn’t feel like Cochrane any more.
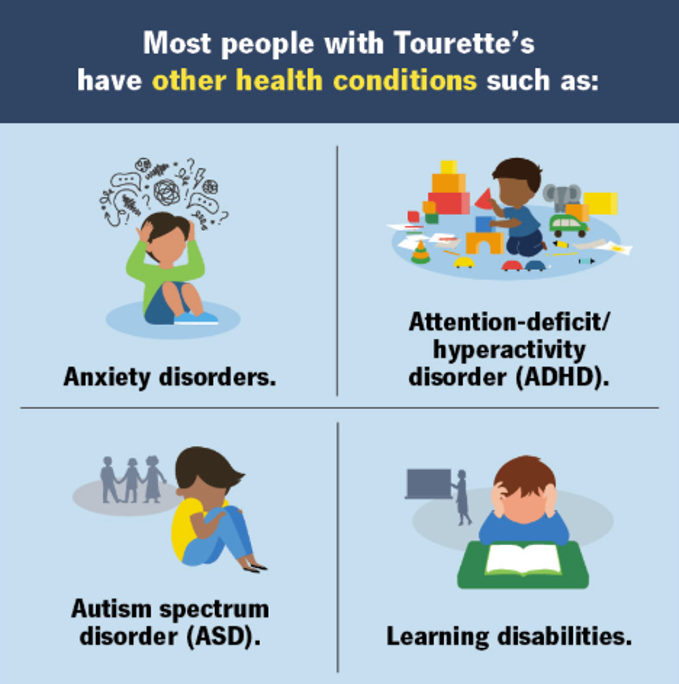
Slide 44: This slide tells you people with Tic Disorders often have ASD and ADHD. Do they? If you have a tic, you are likely to be given a low dose of an antipsychotic which causes loss of focus, You are then given an ADHD scale which asks about focus and diagnoses you as ADHD. You get stimulants which cause tics. Or this scenario can run the other way around. Both of these drugs can cause anxiety or depression so you’ll get an SSRI which – see below – will increasingly give you an ASD diagnosis. In some cases of ASD you may have an intellectual disability. People with Tourette’s were never before thought to have any of these comorbidities. they weren’t drowning in polypharmacy.

Slide 45: This is a graph of UK use of SSRIs for people with ASD. Look at the yellow and purple lines. Yellow is ASD without intellectual disability. Purple is ASD with disability. The use of SSRIs is increasing in both groups – See Sadik et al.
But the Yellow group is more than 3 times larger than Purple group. In other words, most people with ASD now do not have an intellectual disability. The term ASD no longer means people who have had a neurodevelopmental delay. The 18 year old in Holland was unlikely to have classic ASD. Most folk diagnosed with ASD would once have been seen as something else. What?
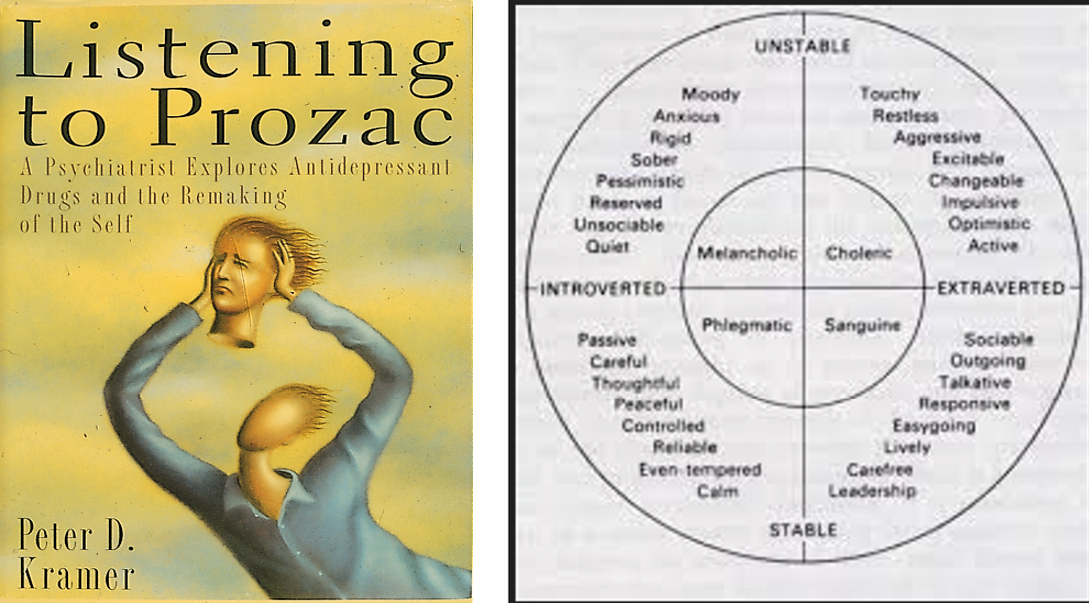
Slide 46: In 1993 the publication of Listening to Prozac was as convenient for Lilly as Driven by Distraction was for them in 1992. The Better than Well responses Kramer featured are much more consistent with an impact on personality than the treatment of a disorder. We can now see this was part of a transition of normal variations in personality into manageble by meds diseases.
Prior to DSM III European psychiatry featured concepts that few American psychiatrists had ever heard of – Extraversion and Introversion. These do not mean talkative and grinning versus shy and sensitive. Extraverts risk take, introverts risk manage. Extraverts share their anxieties around, introverts face them alone. Our personalities shape our responses to meds – introverts respond to SSRIs, extraverts don’t. Extraverts need a very small dose of an anesthetic to put them to sleep for surgery – introverts need much more.
Extraverts are the ADHD folk, Introverts are ASD. Looked at this way the idea we could be both ADHD and ASD at the same time is nuts or lazy.
Just as a football teams need folk who can score goals and folk who can stop the other side scoring we need this variation. Looked at this way, we were better able to use variation – now we are flattening it, making everyone one dimensional.
Folk who have great social skills, who could sell sand to the Saudis and who want to become rich quickly enter corporations thinking that’s the way to go and get set in front of a spreadsheet which they can’t focus on. Their lack of focus becomes ADHD and they get a stimulant which focuses them but kills their creativity and leads to weekend crashes and a disastrous mess.
Slide 47: So what’s going on?
- Real disabilities almost have to be increasing given with the huge increase in meds taken during pregnancy.
- Attempting to suppress normal variation with drugs and labels can only disable more – and is likely to end badly – see image below.
- As is true for all systems, Benefit systems aimed at helping disabled folk are being exploited by smart and well-placed people.
In 416 B.C. Thucydides nailed point 3 down in what has since been viewed as almost the definition of political realism:
The strong do what they can, the weak suffer what they must.
The strong in this case were the Athenians. The Milesians were the weak. It turned out at least as bad for, possible worse, for the Athenians. We have lots of parallels today.
What can we expect from politicians?
annie says
Slide 28: What you are seeing is the best propaganda money can buy – invisible behind the mask of science.
Slide 29: Partnerships like this were evident back in 2004 when the APA were mobilized to resist Black Box Warnings on Antidepressants and wrote an embarrassing suicide note – saying We Believe Antidepressants Save Lives when they should have said Doctors Can Save Lives.
By 2018 NICE was telling clinicians in blunt terms Adult ADHD is real. Statements like the two below close to tell doctors they could be fired if they don’t recognize and treat adult ADHD – which means if the patient says they have it.
Robert Kennedy Jr. continues to promote a plethora of erroneous theories about the origins of autism and AD/HD. These are zombie theories that refuse to die despite their falseness. An important mantra of science is, “In God we trust, everyone else presents verifiable data.”
https://eu.naplesnews.com/story/opinion/2025/04/27/false-theories-about-autism-adhd-promoted-by-rfk-jr-opinion/83237326007/
Grappling with Defence/Welfare Reform do not sit comfortably together. All shades of politicians want to get more young people working, but when asked who they would take off ‘disability’ none have answers, leading to just the ‘feckless’..
ADHD/ASD maybe started as a fad, but is now a colossal Industry which has suckered in young children, teens and adults who seem to sit with their diagnosis.
Another point is if teens with ADHD/ASD are banned from social media, who are they going to talk to and share with?
Obedience – never a truer word from Patrick…
Patrick Daniel Hahn says
Just finished reading Lucifer Curves by economist Rick Nevin. He shows how as blood lead levels in preschool-age children skyrocketed, so did the rate of violent crime — with a twenty-two-year time lag (the average age at arrest of violent offenders in twenty-two). As blood lead levels plummeted, so did the rate if violent crime — again, with a twenty-two-year time lag.
The same pattern held for homicide, burglary, robbery, mental retardation, school dropouts, and unwed pregnancies — all with the appropriate time lag. The same pattern is found in country after country, with preschool-age blood lead levels accounting for most of the variance in violent crime rates.
These findings raise disturbing questions (never answered) about the nature of personal responsibility. How can we hold individuals responsible for their actions when we are flooding their bodies with poisons known to cause anti-social behavior?
Dr. David Healy says
Patrick
The only things that abolish responsibility are delirium and automatisms in a reversible manner so that courts can decide his responsibility was absent at that time. Brain damage by lead is not remediable in this sense – and will lead to permanent incarceration or in the Netherlands or Canada – euthansia. But in brain damage cases responsibility is not usually viewed as abolished – unless for instance there is clear frontal lobe damage.
There can be little doubt that lead causes mental retardation but the correlations you are citing sound a little too ’rounded out’.
David
tim says
How many young and middle aged people cannot work because of the multiple physical, psychological and emotional injuries caused by inappropriately prescribed (often enforced) psychotropic drugs?
Misdiagnosis of SSRI/SNRI/Antidepressant drug adverse reactions (eg akathisia) as ‘Bipolar Disorder”; with inappropriate detention and compulsory ‘treatment’ with ‘antipsychotics’ and ‘mood stabilisers’ results in iatrogenic lifelong, multi-systems disability.
Deprivation of liberty resulting from a common adverse reaction to an inappropriately prescribed antidepressant is unforgivable, and should result in compensation as well as professional accountability for ‘false imprisonment’.
No G. P. is going to correctly certify this iatrogenic cause of not being able to be in employment, education or training. NEET.
Hence, our loved one has not received one single state benefit payment in 16 years of iatrogenic disability.
It seems the options are:
Accept a totally erroneous diagnosis (with its societal isolation and economic devastation) and successfully achieve some State financial support,
For others buying a label such as ADHD in the private sector may seem to be an option?
Accepting a psychiatric label will surely be followed by further exposure to the ADRs of psychotropic drugs.
Appealing to primary care to accept the meticulous EXPERT assessment: –
‘Does not have, never did have a mental illness’ – (from an internationally respected and recognised scientist and doctor) – has at least prevented any further misdiagnosis and maltreatment -(so far).
We are old parents now. What happens when we are not here to advocate for her, and to financially support, love and care for her?
Thank you for another inspirational and important lecture.
Prescribing combination anti-retroviral drugs for pregnant women, to prevent neonatal infection in the early years of our AIDS therapeutic experience, resulted in great anguish re fear of teratogenesis.
chris says
For the victims I think this is the most important and insightful comment. Many relatives have no where near your insights and empathy. Many just want the nightmare of their relatives behaviour out of their lives and will welcome them being drugged into oblivion.
What I would add is that even if your relative did have benefits and savings they would be taxed on Universal Credit starting at 6k and then for every 250GBP over 6k something like £4.35 taxed.
Dr. David Healy says
Chris – Tim
This is an increasingly grim scenario. In addition to I think an increasing amoung of real disability, there are the people disabled by treatments who are now so petrified by their experience at the hands of the medical system that they will not engage with the system – almost even in order to save their lives – and while many will find that incomprehensible, a growing number of us will find it difficult to blame those who’ve been injured in this way.
If you do engage figuring a benefit might help you enter a crazy world where the people on the benefit panel might disagree comprehensively with each other – some thinking that if you have a diagnosis you have a diasability and others not.
Into this mix comes some pretty smart people – who play the system to their advantage.
D
tim says
Thank you Dr. Healy and Chris. Thank you Peter.
In addition to the misery and multiple injuries caused by misdiagnosis of Akathisia, false imprisonment, and a cascade of forced toxic psychotropic drugging – (as every predictable Adverse Drug Reaction (ADR) lead to sequential continued misdiagnoses) : –
There has recently been six and a half hours major surgery (Confirmed serious physical pathology) adding to the suffering, disability and financial deprivation.
The thought of further medical and benefits interrogation is truly horrifying.
The thought of any further unnecessary and inappropriate psychiatric ‘evaluation’ is utterly unbearable.
The surgeon, radiologist and anaesthetist were caring, empathetic, skilful and compassionate. They were all gifted communicators. Initial post-operative intensive care nursing was exemplary. They listened to my fears of AKATHISIA. Several told me that they had never heard of it, as did the Resident Doctor,
Transfer to a busy post operative ward was certainly not an empathetic or therapeutic experience. Perhaps inadequate staffing levels were a factor?
If I had caused the destruction of a beautiful, gifted human being in my own medical lifetime, then I would have been held accountable for my actions and decisions.
Why can there be no accountability once anyone is mislabelled by a psychiatrist who lacks the competence to recognise and manage a common, life-threatening ADR to his/her drugs?
Johanna says
I’ve been trying to get a handle on how this situation is playing out in the USA vs. the UK and EU. Over here, prescription rates and diagnoses of ASD, ADHD, etc. seem to be rising even faster than overseas — but the numbers of folks on public disability benefits such as SSDI and SSI seem if anything to be falling. Of course our “social safety net” has always been less reliable, and is now being cut to ribbons.
Personally, I seem to meet ever-larger numbers of adults, especially younger adults, who identify as “neurodiverse.” But few if any of them are on disability. Sounds like you are encountering quite a bit of the same (bright and fairly “together” young adults who insist they have ASD, ADHD or both).
So I am very interested in Slide 40! You describe it as showing both the rising numbers of folks on disability, and their plummeting average age. But the slide itself states it shows the “Age Profile in Despair, 2009-2022” in the USA, from the Behavioral Risk Factor Surveillance Survey, a phone survey by the US Centers on Disease Control (CDC). Self-reported feelings of “despair” are way up since 2019, it shows, and the peak age for despair has shifted from about 50-52 to about 20.
Is this slide from the US or UK? Does it actually pertain to disability? And if not, is there another one that does?
Dr. David Healy says
Jo
Well spotted. I have two graphs confused. This one as you note refers to declining wellbeing and is US. It features in along with the document it comes from linked into the Damsels in Distress post on DH – May 9 2024.
The DiD post refers back to The Great Silence post March 2024 , which has the graph I thought I was quoting.
The debate over here has got pretty febrile. It is interesting that US disability benefits which surged 20 years ago leaving George W claiming that social welfare needed to be privatized or the US would go bankrupt. I guess its no surprise that this has happened but what is surprising is that so little is heard about what exactly happened and how it was engineered.
David
Johanna says
Thanks! The uptick in Social Security Disability in the 2000’s and 2010’s was definitely centered on middle-aged workers, especially men. The prescription opioid epidemic was a big driver of this. People who would once have recovered, at least sort-of, from injuries and ailments now never returned to the workforce. And some were directly ruined by addiction.
The simultaneous attack on workers’ compensation made it worse: people who once could have counted on either a modified job, or a decent settlement were left shipwrecked with public SSDI and Medicare their only refuge. We heard a lot about “deaths of despair” as you may recall: drug overdoses, suicides, alcohol-fueled deaths.,
Will try to find out the actual numbers re: young adults not in the workforce! Depression, and prescriptions of psych meds to the young surged during the pandemic — but were pretty damn high already. Not sure if the rise in new autism diagnoses has led to more prescriptions (or for what drugs). And the current slashing of food and medical aid programs is supposed to “put people back to work,” but most of us suspect this is just a crude pretext.
Dr. David Healy says
There was a rapidly rising use of psych meds by the young pre-pandemic. I think the pandemic has served as a semi-plausible excuse for what has been happening.
D
Harriet Vogt says
What can we expect from politicians?’
Alan Milburn, lead author of the – ‘independent’ – interim report on ‘Young People and Work’ is, an extremely skilful one and a commercial business success. Plus, one suspects, the eminence grise behind a lot of the UK’s health and social policy strategy, Labour’s political enfants terribles can’t really cut it – though Wes went up slightly in my estimation when he was both sympathetic and decisive in instigating the Nottingham and TEWV investigations into deadly failures of the ‘mental health’ system. The new guy – as you likely know, Wes bailed before Healey ,in the hopes of winning a leadership contest (he won’t ) -is a nodding dog. ‘Transwomen are women’ – nod, nod. ‘The Supreme Court ruled only biological women are women’ – nod, nod.
I raced through ‘Young People and Work’ it is curious the way these public policy documents – cf the UK’s Suicide Prevention Framework – aren’t wrong – they cover all the obvious surface metrics, demographics, socio-economics, measurable behaviours, system delivery etc. But they are strangely devoid of insight. They tend to produce organogram thinking, rather than drive cultural change. But then how do you do that – I haven’t thought that one through…
.
Being the party of access, Labour cannot and will never say – this youth crisis is in significant part the result of the confluence of commercial opportunism, a market share grab from biomedical psychiatry and government collusion – serving up a generation of young people who are hamstrung by self-perceptions of ‘mental health disability’ -notably depression, anxiety, ADHD and the more fashionable, less serious neurodevelopmental end of ASD.
It’s far too late for that anyway– as we know these diagnoses are now socially embedded and valued, often actually valuable, aspects of identity. Whereas once they were rare and undesirable conditions no one wanted to own.
Milburn et al have done a relatively deft workaround. Key points – ish:
1.No probing questions about the ‘mental health’ suffering of the young – it’s real. A nod to the diagnosis – medicalisation polarisation – but no engagement. Certainly, no direct mention of drugging and iatrogenic disability.
‘The public discussion of these trends has become heavily polarised. Some emphasise under-recognition and demand more diagnosis. Others raise concerns about over-diagnosis and medicalisation. This review does not align with either camp.’
2. Recognition of the obvious – ‘mental health’ problems are upweighted to deprivation, biased to some ethnicities, poorer GP services in poorer areas etc. Health and social care policy is big on the ‘health inequalities’ mantra – like ‘lessons being learned’ – but what changes? Not a lot. As a heathen, I wonder if this is like religious incantations – the doing is in the saying, not the doing.
3. A central issue – healthcare/GPs only treat these problems as acute (drugging) and not integrated with whole productive lives. There is a hierarchy of ability to work within disability– and at the moment these are amorphized, We need to develop prevention strategies and positive work opportunities to drive change. Oh ,and social media comes in for a ritual slap – but then that’s about to be banned for under 16s. Another discussion.
Hmm – they’re right about a sort of stratified disability/ability to work, in theory, But -just imagine how this is going to play out in practice. Who will decide on the levels of disability? How will iatrogenic disablement be managed? Patients struggling with antidepressant withdrawal or psychotropic adverse effects already have to fight bitterly for state support. How will they prevent ‘anxiety’ ‘depression’, ADHD, ASD? Will this involve ‘mental health screening’ with normative scales like Pritzker is /was mandating for Illinois? Then what? How will they motivate more GPs to work in areas they don’t fancy? And,.And. And.
I suppose a big part of the answer lies in the educational and occupational temptations they dangle at NEETS.
‘The question the system should be asking has to move from “how many young people have a condition” to “what enables young people to remain engaged in education, work and ordinary life”.
You’d hope the answer will be in Part II.
Female ADHD. Don’t, as they say, get me started This is an infuriatingly stupid sell for female ADHD:
‘How to spot ADHD in women in 25 seconds. They will have a huge amount of internal chatter, a million thoughts happening simultaneously – and this will cause paralysis and stop them from able to do anything so they may be lying on the sofa scrolling social media and this will look like laziness but it’s not they’re literally unable to do anything else right now . They will have an intense fear of rejection…blablabla’.
https://www.tiktok.com/@adhd_chatter_podcast/video/7374762137614322976?lang=en
It’s quite clear to me, as to many others, that ADHD is not a thing – but variations on a cognitive style that works fabulously well in creative and entrepreneurial environments. And we all know it’s massively over-diagnosed in the young for year –literally the less mature. https://www.nottingham.ac.uk/news/adhd-and-school-age-study
Stop dishing out Patrick’s obedience pills – and fit the environment to the child and the person.
Dr. David Healy says
H
Samizdat hopes that Patrick’s Obedience Pills – the book – get’s dished out more and more.
There may be a tiny sliver of hope in that we don’t hear as much about Bipolar Disorder these days – it’s not as “fashionable”. These epidemics (aka Fashions) made in marketing departments come and go – they have to.
The worry in this case is that while the fashion might go and it’s no longer fashionable to loudly proclaim I’m Bipolar, you get left on and can’t get off the meds that went with the fashion. A bit like a tattoo. Complicated when you have the name of a previous boyfriend or girlfriend featuring prominently on your arm
D
Harriet Vogt says
Patrick’s book – ‘Obedience Pills’ – with that graphically fabulous cover (Bill again!) – has now supplanted Andrew Doyle’s – ‘End of Woke’ – in my reading list.
I’ve been an ‘ADHD’ iconoclast for many years – after watching Louis Theroux’s classic documentary, ‘America’s Medicated Kids’. The kids were great – their teachers, parents and especially psychiatrists collectively round the bend.
https://www.bbc.co.uk/programmes/b00s56gx
I’d guess the marketing thinking must be to focus on the diagnoses that are closest to accessible, mass market consumer goods – not too specific or weird, so widely relatable as lifestyle identities with drugs attached, All those generic license holders need volume sales. Bipolar is a bit too serious and niche– and I don’t see many queuing up for a life of ‘Schizoaffective’ Disorder’ whatever nonsense that is. Ofc the fact that getting off the pills is hell for many, and worse for some, is the ultimate customer loyalty mechanism.
I used to have a recurring nightmare – no longer, thankfully. I was in an endless, tight, rectangular tunnel on my hands and knees, trying to keep a huge, heavy roll of metallic material smooth and straight, behind and before me. Ofc it kept rolling back – relentlessly. This feels relevant.
Dr. David Healy says
H
Bipolar was a seriously illness but for a decade from 2004 – anyone could have it in fact almost certainly had it but just didn’t know it.
One of the fashions I found mystifying at first but now accept that it’s a happening thing is people embracing the idea they have a personality disorder and celebrating it.
Even schizophrenia – as in split personality or the American/Freudian understanding of it could come back into fashion as dementia praecox is really disappearing
One of the most famous phrases in medicine is the art of diagnosis is about cutting nature at its joints. In mental health its much more like taking a cookie cutter to the dough of nature
D
D
Harriet Vogt says
I’ve taken a quick trip to Cookie Cutter World aka TikTok. Dystopian doesn’t come close.
Just looking at the numbers of TikTok hits for the most popular ‘mental health’ diagnostic hashtags – ‘#Anxiety’ and ‘#Depression’ vie for first and second place with,respectively, 35 and 40 BILLION. ‘ADHD’ 14 billion, ‘PTSD; 11 billion, ‘Borderline Personality Disorder’/#BPD romps home with an impressive 3.7 billion (particularly impressive since it’s a female diminishing load of garbage) – way ahead of ‘Bipolar’ at 2 billion, currently, as you noted, falling out of fashion – and some other cocktail of weirdness #DID (Dissociative Identity Disorder) 1.5 billion. Schizoasffective disorder is a bit more niche, but still gets plenty of hits. There is even a more broadly based genre of disjointed music- Schizomusic.
Cookie Cutter World is a pretty disturbing destination. Beautiful, articulate young women like @letterfromliv conceptualise their perfectly ‘normal’, for lack of a better word, emotions as inexperienced, arguably over-introspective young women as ‘BPD’:
‘Having a BPD diagnosis is a really strange experience because you go through all of the things that you have no words for and the you go through the list of symptoms and things like chronic emptiness, fear of abandonment , idealising , devaluing – they all have names –like they’re all mechanisms, they’re all things that are actually happening and I feel like a spent so long thinking I was categorically insane…’
https://www.tiktok.com/@letterfromliv/video/7646680840381959446?q=%23BPD%20EXPERIENCE&t=1782346624583
https://www.tiktok.com/@schizokitzo is pretty wild and makes loads of -um-educational videos. Diagnosed with ‘Bipolar type Schizoaffective disorder’ (is this even a thing – or have they mixed up the cookie cutters?) – for which she takes what sounds like a picnic hamper of drugs everyday. Quite a lot of others in the ‘SA’ community ask her questions about adverse drug effects, e.g.
‘Hi I have skitzoaffective (sic) disorder. I take haldol and have EPS. I have trouble walking fast, I can’t get on a treadmill, I can only walk slow or else I get cramps in my foot. Did you ever experience this?’
To which she seems to give honest, helpful answers, all delivered with a particularly chemical kind of intensity:
‘At first I ended up in emergency – why are my legs not working hands shaking? Some people take levodopa, mine is an anticholinergic medication I used to want to be a surgeon- definitely not possible now. (she demonstrates the constant tremor in her hands).’
I think we all grow weary of smartarses intoning – correlation isn’t causation – but in TikTik Cookie Cutter World it most certainly is. Are we even remotely surprised that diagnosed and drugged young women especially lead the misery and suicide index in Danny Blanchflower’s imo uninsightful work?
So many, including our pathetic UK government, imagine that the solution is to block social media access for kids until they are 16. (at the same time as being happy to subject 220ish 11 and 12 years olds to puberty blocking chemicals to do gender ‘science’ aka politics). The libertarian in me bridles at blocking social media for kids- it is the world we all live in. But, equally, there is some sense to it – limited early access to ‘mental health’ identities – maybe.
The point is, perhaps, that we need to be creating a social framework of positive values, more than just banning access to the dodgier elements. There was a fantastic example of how to do this a few months ago – the emotionally connected young mayor of Genoa, Silvia Salis, helped organise a free open air concert played by a famous Belgian techno DJ, Charlotte de Witte. Social cohesion and pure elation. #Amazing.
https://www.instagram.com/reel/DXAdWWKiYjk/?utm_source=ig_embed&ig_rid=AqwbjQbnlwFS7QIf-4qDX4n
But then Italy has always had more of a framework of positive family, cultural and I guess, to some extent, still religious values. Is it mere correlation that Italy has consistently lower antidepressant consumption than the OECD average?
https://pmc.ncbi.nlm.nih.gov/articles/PMC12213856/
I have to admit that – despite being thrilled by the spirit of the Genovese concert – my visit to Cookie Cutter Land put me more in mind of an old bloke who used to walk up and down Oxford Street in London wearing a placard saying, ‘The end of the world is nigh’. I expect the poor chap has keeled over by now – but, if not and I ever come across him again, I’d say, “it’s alright mate – you can put that damn thing down now. The end of the world has just happened on TikTok’.
Dr. David Healy says
H
This is a truly fabulous comment.
It catches the growing lunacy of our times
The shame of it is that so many of the brightest and the best (young women) are caught up in the lunacy.
It feels like a Euripedes Medea moment.
D
Jo Ann Cook says
I am forwarding your excellent article to a few politicians, one in particular who is considered progressive and recently submitted a bill for mental health parity.
It is scandalous. This twentieth century evil was predicted by Aldous Huxley in his book Brave New World.. Huxley envisioned a terrifying future in which the sciences would be used by biologists and psychologists to rationalize the destruction of normal emotions and behaviors in children through biological and chemical engineering.
Dr. David Healy says
JoAnn
We need to be careful here. Biology is a source of variation and individuality. It isn’t it that’s trying to destroy normal emotions and behaviors. Social forces are doing that – social techniques like randomized controlled trials that average us.
David
David Healy says
The BBC reports June 29
Michelle Roberts Digital health editor
The number of children referred to mental health services in England has risen by 10% in a year to more than one million, according to a report. The latest data from 2024-2025 is almost double the number in 2018-19.
Anxiety was listed as the most common reason, accounting for 16% of all referrals, while cases of suspected autism rose by almost 50% in a single year, to more than 96,000.
Other neurodevelopmental conditions, such as ADHD and Tourette’s syndrome, also increased – by nearly a quarter.
In her annual report, Children and Young People’s Mental Health Services: 2024-25, Children’s Commissioner Dame Rachel de Souza warned that increasing numbers face long waits for support.
Over a third of the children were still waiting for treatment, with more than 60,000 waiting over two years for help – an increase from over 44,000 children the previous year.
Fewer than one in five with suspected autism or neurodevelopmental conditions went on to receive treatment in 2024-25. Those who did waited, on average, a year for support.
Dame Rachel called the figures “stark”, saying that while there had been some improvements, with more children receiving support last year, it was hard to ignore the “colossal challenge” facing mental health services, as demand outpaces system capacity and funding.
She said there needed to be a shift in approach, with greater focus on joined-up services “across health, education and social care to ensure children are getting the help they need in schools and the community”.
The charity YoungMinds said it was extremely concerned about the additional barriers and waiting times some were experiencing, particularly by black and racially minoritised children and young people, as well as those referred to services with suspected autism or neurodevelopmental conditions.
The figures show that black and Asian children are underrepresented in referrals and that when they are referred, they are much more likely to be in severe distress or crisis. One in four black children directed to children and young people’s mental health services were referred for being in crisis, compared with 16% of Asian children and 7.4% of white children – raising questions over why some children from ethnic minority backgrounds are not receiving help earlier. Children from the poorest 10% of areas in England made up 15% of referrals, compared to 7.6% from the least deprived areas.
Dr. David Healy says
Posted on BBC on June 28
TV personality Hayley Pearce is pregnant with her first child and wondering how her “neurospicy” brain will handle all the demands of motherhood. The 36-year-old, who shot to fame as the tea lady in BBC Three fly-on-the-wall series The Call Centre, was diagnosed with ADHD at 20. “I have no concept of time… I’ve been sacked from jobs because I’m always late,” she said. “I’m not an organised person… I’m overwhelmed all the time.” She said her midwife had told her that her ADHD means she may be more likely to have postnatal depression than someone who is neurotypical.
Hayley hopes that by sharing her experience of ADHD it will start a conversation about how women like her can be better supported. Hayley’s home in south Wales is currently full of sticky notes to help her keep on top of everything she has to do. “I’m overwhelmed right now with too many appointments going on,” explained Hayley, who now works alongside social services with looked after children.
“I am neurospicy as I like to call it. I’ve always been like 100 miles an hour, some people call it scatty.” Hayley’s TV career started when starred in the BBC reality TV series The Call Centre in 2013 and went on to make a number of documentaries and host a podcast
According to the NHS, symptoms of attention deficit hyperactivity disorder (ADHD) can include being easily distracted or forgetful, finding it hard to organise your time and finding it hard to follow instructions or finish tasks. It is something Hayley, who was diagnosed a year before rising to fame in The Call Centre in 2013, has lived with for as long as she can remember.
Hoping to pick up some tips on how to stay on top of everything once her baby comes along, Hayley went to meet 42-year-old Rhiannan Morgan. Rhiannan has four children with autism aged 21, 14, 11 and nine. Like Hayley, she has ADHD. “Every time I was about to have a baby I was thinking ‘well if I don’t get my act together now I’m in real trouble’,” she said.
When her children were little she spent many hours online looking for strategies to cope. Rhiannan creates resources to support what she calls other neurosparkly mums and families. The result is a range of hacks she uses to stay on top of everything. Posting on social media as Mummy of Four, Rhiannan also shares tips online and creates resources to support what she calls other neurosparkly mums and families.
“ADHD brings lots of creativity and enthusiasm,” she said. “But it also brings challenges with working memory and remembering things and if you don’t have those systems and strategies in place it just feels like you’re trying to swim uphill constantly.”
Rhiannan has ADHD and has developed a range of hacks to help her stay organised
Some of the hacks that Rhiannan says help her stay organised, include:
• Ask children early on to help with household chores
• Write a weekly meal plan
• Encourage children to help with shopping list
• Set up comfortable area to feed baby with comfortable chair, water and phone charger
• Put information from letters and emails straight into your calendar and pay bills immediately
• ‘Set and forget’ such as having groceries delivered on same day and time every week
• Use alarms on mobile phone as prompts to do tasks on time
• Use a screen time app to avoid being distracted
Another concern on Hayley’s mind is postnatal depression after a Swedish study of more than 770,000 births indicated mothers with ADHD could be up to five times more likely to experience postnatal depression than those who are neurotypical.
Dr. Nicola Peek, a counselling psychologist in the Perinatal Mental Health Service at Hywel Dda University Health Board, said this is because women with ADHD are more sensitive to the sharp drop in oestrogen and progesterone that occurs after childbirth, which can cause a dip in dopamine levels.
“They might present as feeling lower in mood, more fatigue, more brain fog, they might find it’s difficult to focus on things in the way that they used to,” she said.
Dr Peek’s advice for new mums with ADHD, includes:
• Advocate for yourself when engaging with medical professionals
• Remember that social media can set up a lot of unrealistic expectations and what others share is not always the reality
• Talk to your partner, family and friends about how you’re feeling
• Have boundaries with others around things such as advice giving
“With ADHD you can be an incredible parent,” she said.” “There’s going to be huge empathy, there’s going to be huge creativity.”
Hayley says she loves many things about having ADHD, such as being a “fun auntie” With Hayley’s baby expected in just a few weeks’ time, she is determined to keep talking to those around her about how she is feeling. “If I struggle, I struggle, I’m going to be honest about how I feel,” said Hayley, who lives in Maesteg, near Bridgend.
“My life’s going to take a massive 360 when I have this baby. “It’s going to be testing, it’s going to be challenging and it’s probably going to be the best feeling and the best thing I’ve ever done in my life.”
Harriet Vogt says
Heartsink skimming your latest comments – which I will read properly later. This is a slightly frivolous reply to our earlier deadly serious exchange.
I looked up the doomsters of my youth. I rented a fabulously cheap flat in the ‘industrial bin’ end of Mayfair, just behind Oxford Street and a stone’s throw from Speakers’ Corner- it was the analog version of today’s doomscrolling.
I expect most of us came across the standard issue, grim faced blokes with – ‘The end is nigh – repent ‘ sandwich boards – lurking around most towns. I always wondered what ‘nigh’ meant since the same chaps seemed to have been issuing this same dire warning for years. Of course, we know that – NIGH – is finally upon us.
But, my research reminded me of another character I saw a lot in my local manor, Oxford Street, a certain Stanley Green. Stanley had been in the Navy in WWII and was maiden aunt shocked by the unbridled lust exhibited by his fellow sailors. He put this down to an excess of protein. So Stanley – whom I remember clearly – marched up and down Oxford Street between 1969-1993 with a sign saying, ‘Less passion from less protein – (specifically) fish bird meat cheese egg peas beans nuts. And sitting’.
https://www.bbc.co.uk/news/uk-england-london-66853581
I expect he might have been an SSRIs enthusiast with their passion deleting potential – but dubious about keto.