
In a recent press conference, Emmanuel Macron said that France faced a Fertility Crisis and needed a Demographic Rearmament – see Liberty, Equality, Fertility. The Timeline below traces an important contribution from the medicines we take to that crisis, left unmentioned in his speech – and the role of an important player, the Industry making those medicines.
The Early Years
1930 French pharmaceutical companies made a speciality of research on antihistamines, many of which are now known to be serotonin reuptake inhibitors. These were the blockbuster drugs of the 1930s. It now looks like French laboratories created thalidomide before World War II. Thalidomide and SSRIs share common effects on sexual function, pregnancy, suicidality and peripheral neuropathy, with some shared mechanisms linked to these effects.
1952 French psychiatrists discovered the effects of Chlorpromazine, an antihistamine. This became the first antipsychotic and led to a flood of similar compounds – all endocrine disrupting – perturbateurs endocriniens. In the Sainte Anne Hopital, below in the dark coat is Jean Delay with Pierre Deniker on his left whose nursing staff make the crucial observations and Pierre Pichot on his right. See interviews with Pichot, Lemperiere on Pichot’s right and Thuillier on her right. For another view see Pierre Simon.

1956 Thalidomide migrated to Germany in 1954. The first evidence it caused birth defects was the baby of a member of staff in 1956. For 6 years and more Chemie Gruenenthal flat out denied it could cause problems.
1958 The first Tricyclic Antidepressant (TCA), Imipramine, derived from an antihistamine and modelled on chlorpromazine, launched. It was followed rapidly by Amitriptyline, Trimipramine, Clomipramine and later more selective noradrenaline reuptake inhibitors, Desipramine and Nortriptyline. Depression at this point is a rare disease. Pharma has little interest in it.
1960 A Randomized Controlled Trial (RCT) by Louis Lasagna shows Thalidomide is Safe and Effective.

1960 Frank Ayd reports Amitriptyline, his drug, can cause sexual dysfunction. Ayd found it easy to spot this even though melancholias (severe depression) being treated then also caused loss of libido. Doctors now cannot spot SSRIs causing more obvious sexual problems in conditions that themselves do not cause sexual dysfunction.
1961 Discovery of the anticonvulsant action of Valproate, in Lyon.
1961 Discovery of the role of SRIs in Obsessive-Compulsive Disorder in Lyon.
1962 In response to a Thalidomide birth defect crisis, the US Drugs Regulator, the Food and Drugs Administration (FDA) put RCTs in place to ensure Thalidomide problems do not happen again – the same RCTs Thalidomide looks perfectly safe in.

1966 Discovery of Valproate’s mood-stabilizing actions in Lyon
1968 Students protesting in Paris in 1968 ransack Delay’s office. From Japan to the US, biological psychiatry was seen as a problem. The camisoles chimiques then, now they make us Better than Well.

Photo from 1968 Magnum Photos.
The SSRI Years
1968 Arvid Carlsson establishes Clomipramine, Amitriptyline and Imipramine as Serotonin Reuptake Inhibitors (SRIs). They are not selective to serotonin – would be called SNRIs now – but stronger than SNRIs and less side effects, perhaps because of their anticholinergic actions. Desipramine and Nortriptyline are selective noradrenaline reuptake inhibitors.
1969 Carlsson suggests making a selective serotonin reuptake inhibitor.
1970 Clomipramine (SRI) emerging as the most effective antidepressant. Carlsson creates Zimelidine the first selective SRI – an SSRI – adapted from brompheniramine an SRI antihistamine.
1973 Clomipramine and other SRIs used for Premature Ejaculation (PE). Only 10% of an Antidepressant dose 30-60 minutes before sex is needed to help – it numbs penis and delays orgasm.
1975 Clomipramine established as the best treatment for Obsessive-Compulsive Disorder (OCD).
1980 Valproate causes birth defects.
1982 Zimelidine launches in Europe. It is withdrawn 3 years later because it appeared to trigger Guillain-Barre syndrome in rare instances.
1983 First cases of SRI withdrawal induced persistent genital arousal disorder (PGAD) noted by Isaac Marks researching Behavior Therapy for OCD and finding people stopping their Clomipramine could have enduring sexual problems.
1984 Indalpine launches in France, Citalopram in Scandinavia, and Fluvoxamine in Belgium and Europe. All are SSRIs. Indalpine withdrawn 2 years later because of liver problems.
1985 Danish clinical trials show Clomipramine more potent than new antidepressants like paroxetine (a Danish drug). Is it a problem for companies producing an SSRI that is less effective and more expensive than older drugs? No. The older drugs are for severe diseases – we are aiming at the worried well and offering to make them Better than Well.
1985 Beecham, later SmithKline Beecham, later GlaxoSmithKline (GSK) Healthy Volunteer Phase 1 Study shows Sexual Dysfunction the worst side effect on paroxetine (later Paxil, Seroxat, Deroxat). Over 50% badly affected with some post-trial effects.
1985 Volunteers like Traci Johnson below in company SSRI Phase 1 trials – viz fluoxetine, sertraline, duloxetine, paroxetine studies commit suicide, become aggressive, become dependent after exposures of only 2 weeks.

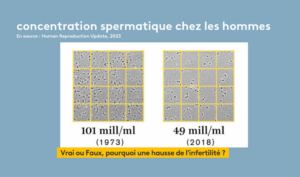
1985 Western Male Sperm Counts Falling. Have more than halved between 1973 and 2010.
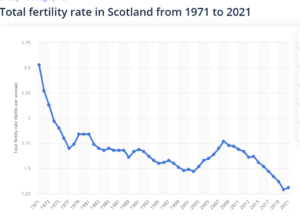
1985 Western Fertility Rates fall below the 2.1 Reproductive Replacement Rate. Scotland below is the country with the highest SSRI consumption in the UK and its fertility rate is now 1.3.
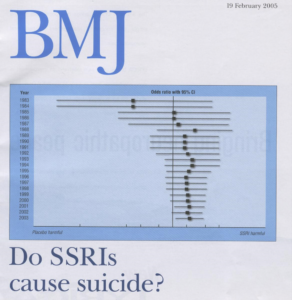
1987 By 1987 published SSRI trials show an excess of suicidal events on SSRIs.
1988 Having failed in efforts to market Prozac for hypertension or weight loss, Lilly begin ‘antidepressant’ trials. Marketing as an antidepressant has become an option because there is too much adverse publicity about dependence around benzodiazepine anxiolytics – tranquilizers. Drugs like Buspar have proven doctors won’t buy the idea of a non-dependence producing anxiolytics.
Lilly launch Prozac in the US, somehow generating the impression it will among other things cause weight loss. Later marketing spins it as making you Better than Well. We have known since the 1950s that drugs that cause some of us to commit suicide can make others feel Better than Well.
1988 Regulators and Companies get reports of Post-SSRI Sexual Dysfunction (PSSD)
1990 Teicher et al report convincing evidence Prozac causes suicide. Many other groups report similar findings including Healy and colleagues.
1991 Lilly invite Healy to be a consultant for them and among other things ask his opinions on how doctors and the public would view developing Dapoxetine, a short acting SSRI, for Premature Ejaculation.
1991 Human Fertilization and Embryology Act set up in Britain to license IVF services for women. IVF – in vitro fertilization. ART – assisted reproductive technologies. AMP – assistance medicale pour procreation.
1991 At launch sertraline (Zoloft) and paroxetine (Paxil) claim less than 5% of people in clinical trials have sexual issues and no mention of symptoms on stopping (SoS).
Lilly, Pfizer and SmithKline breach FDA regulations manipulating their clinical trial data to hide suicidal events. FDA staff write memos that FDA heads ignore.
1991 SSRI labels mention nothing about genital numbing, which affects 90+% – or genital irritability which can lead to PGAD. This irritability appears in the media linked to Prozac and is portrayed as a benefit – Prozac can give you more orgasms than you have ever had before. Yawn and you can have an orgasm.
1991 Genital numbing demonstrated on electrophysiology with clomipramine.
1991 The branding of crazily over-potent serotonin reuptake inhibitors as SSRIs originated in SmithKline’s Marketing Department, along with a resurrection of an idea about low serotonin being responsible for depression that had been discarded by science in the 1960s.
1992 Extension of IVF to men with poor quality sperm.
1993 Independent studies show up to 90% of people on antidepressants have significant sexual issues.
1993 SSRIs like paroxetine rapidly begin being used for Premature Ejaculation.
1993 GSK tell Investigators in Clinical Trials – Do not ask about Sex.
1994 Regulators have more reports in 3 years from doctors reporting paroxetine induced dependence than they had reports for benzodiazepine dependence over the prior 20 years.
1999 Withdrawal study shows 50% enduring sexual dysfunction on stopping SSRIs
2000 Healy sees his first case of PSSD. Some have had PSSD for 10 years by then.
2001 First academic article on PGAD – Leiblun and Nathan.
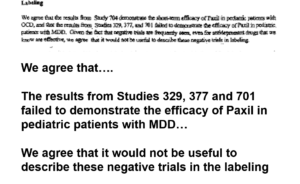
2001 Study 329, a study comparing paroxetine to placebo in depressed teenagers, is published.
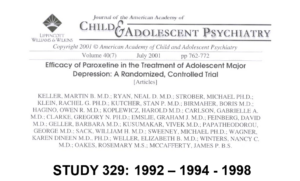
2004 SSRI get a Black Box Warning for Suicide and Aggression. New York State lodge a fraud action against GlaxoSmithKline centered on Study 329 claims paroxetine works for depressed teenagers when it doesn’t.
{kind=link}
It appears that:
- Almost the entirety of the pediatric antidepressant literature is ghost-written
- The gap between company efficacy and safety claims and the data is total
- Regulators like FDA know that published articles are false.
SSRIs Sex and Fertility
2004 National Toxicology Program report Prozac Rat Sexual Toxicity Study – Prozac wipes out male sperm and produces testicular toxicity.

2005 Prilogy (Dapoxetine), an SSRI, launched for Premature Ejaculation.
2005 FDA Guide for Industry on how to establish cause and effect relations between company drugs and adverse effects use the known effects of SSRIs on sexual function as an example.
FDA Guide for Industry on Good Pharmacovigilance Practice also uses the known effects of SSRIs on sex as an example.
2006 First academic articles on PSSD – Bahrick, Csoka and Shipko.
2007 European Regulators question Lilly about the Rat Study on Prozac and Male Sperm. They are concerned about the implications for Fertility – Cradle of Civilization.
2008 Senator Grassley brings PSSD to FDA’s attention who tell him they are impotent when it comes to deciding if SSRIs cause PSSD – Healthcare Gone Mad.
2009 The Kilker Trial gives a verdict against GSK in a case involving paroxetine and birth defects. These verdicts lead to hundreds of other settlements likely costing GSK somewhere around $1 billion. The evidence presented shows failure of implantation, increased rates of miscarriage and birth defects linked to SSRIs. The evidence later shows SSRIs cause behavioral defects in children and trigger alcohol abuse during pregnancy leading to Fetal Alcohol Syndrome in children.
Few doctors in the Western world get to hear about Paxil on Trial. A demonstration of pharmaceutical company abilities to shut down bad news.
2011 First academic article on Post Finasteride Syndrome (PFS) – a clinical condition closely related to PSSD caused by Finasteride – Propecia, a drug taken by teenage boys and young men to prevent hair loss.
2012 Regulators require Medical Label change to mention SSRI effect on Fertility. Companies do not add Fertility concerns or PSSD to Patient Information Leaflet.
2012 Growing reluctance in the media or medical journals to mention Sexual Effects or any Adverse Effects of SSRIs. We do not want to deter people from getting the benefits of antidepressants. Social media campaigns against pill shamers start.
2012 5 + million babies born by IVF – mainly Western.
2012 James Holmes Aurora shootings at the premiere of Dark Knight Rises – kills 12 injures 70. His plans to shoot people all emerge after he is put on Zoloft.
2013 DSM 5 mentions Post Treatment Enduring Sexual Dysfunctions.
2014 First mention of Post Retinoid Sexual Dysfunction (PRSD) triggered by isotretinoin – Accutane – in the academic literature. Another clinical condition closely related to PSSD. Isotretinoin is taken by young people for acne.
2015 Restoring Study 329 is published.

2015 Up to 15% of Western populations take SSRIs, making them effectively Infertile or at risk of complete loss of sexual function (PSSD) if they manage to stop treatment.
2016 Valproate causes transgenerational birth defects.
2018 RxISK petitions FDA and EMA re PSSD – FDA still sitting on it
2019 BMJ feature article on British people (and Westerners) not having sex as much as before. In the previous decade, there has been a rise in Asexuality, which in animals can be linked to SSRI intake during pregnancy. BMJ article blames depression but the worried well states that lead to antidepressants do not cause a loss of libido – SSRIs however do.

2019 EMA add PSSD to medical section of SSRI labels – not to patient information leaflet. RxISK has laid out in several posts just why EMA and FDA find it difficult to link drugs to adverse effects like PSSD – because they are bureaucrats. It is not their job to interview patients.
2020 Children of the Cure published – the background story to Study 329.

2021 Romain Schmitt dies while taking paroxetine – Deroxat. His parents find French doctors have difficulties blaming prescription drugs for any problems.
2021 Health Canada add PSSD to Antidepressant labels – but not to patient information leaflet.
2021 1-3% women have PGAD – SSRIs the most commonly identified trigger.
2021 100+ IVF clinics in the UK – 10+ million IVF births globally.
2021 La Peau des Pêches is published – puts Infertility on the map.

2022 Up to 6% of people may have PSSD on stopping SSRIs.
2022 Diagnostic Criteria for PSSD and related Sexual Dysfunctions published.
{kind=link}
2022 Boston RCT shows Antidepressants not Depression leads to male infertility.
2022 PSSD network set up. For the first time, people put their names and faces to PSSD. The network starts engaging vigorously with Social Media.

2022. New York Times reports a growing number of American teens are on a growing number of psychotropic drugs – some on up to 10 meds.

2023 Spain, Italy, Japan, many European countries have Fertility rates below 1.30 Native Fertility Rates may be as low as 1.0 – in Britain women born outside the UK are having 30+% of babies.
2023 HCFEA in France reports that an increasing number of French young people are on psychotropic drugs. The response from psychiatry is this shows lots more children need help with SSRI and related drugs.
2023 Close to 30% of Spanish 18 year old girls are taking psychotropic drugs. Most countries report a huge increase in psychotropic intake among teens and children in recent years – commonly blamed on the Covid pandemic. This Spanish site links inequality in psychotropic drug intake to gender inequality.
2023 Extraordinary PSSD network podcasts about PSSD – Roy, Bryn and Simon , Rosie, Emily, Daryl, Carlton and others. Rosie triggered The First Podcast.
2024 Nobody taking an SSRI is warned about Sexual Dysfunction or InFertility – the sexual and fertility effects of SSRIs are much more common than mood benefits.
2024 IVF rates approaching 10% in Scandinavia and Japan.
2024 Medical Assistance in Conception (MAiC) and Medical Assistance in Dying (MAiD) rates roughly equivalent in countries that have both.
2024 Emmanuel Macron launches a Demographic Rearmament campaign.

Between killing libido, and killing sperm, SSRIs may be the single biggest cause of infertility. They are increasingly an obstacle in the way of anyone wishing to remedy National Fertility Problems. This problem cannot be remedied if people are kept in the dark about these and other prescription drugs.
In his recent launch of a Demographic Rearmament program see Liberty, Equality, Fertility, aimed at supporting French Fertility, which seems to have taken inspiration from Salome Berlioux‘s La Peau des Pêches, Emmanuel Macron focused on making it financially possible for younger women or couples to have children. And also on the risks of Petrochemical – pertubateurs endocriniens – endocrine disrupting chemicals.
Fifty pages of the key report behind his press conference are given over to or mention these Petrochemicals, some of which are endocrine disrupting by accident.
One page mentions prescription drugs, medications sur ordonnance, which are endocrine disrupting by design.
Is this a bias to which we all succumb? We locate the dangers in life, the rapes, the abuse, the violence, in strangers – immigrants, chemicals we can’t see or recognize. But in fact again and again, the actual harm comes from familiars, people we know. The chemicals in shiny capsules we take every day that are given to us by the reassuring figure of a doctor.
See Medico-Chemical and Petro-Chemical Twins.
RxISK knows of 18 people who have taken their own life with or without Medical Assistance because of PSSD in the last 2 years. There are likely many more.
mary H. says
This post reminded me of one morning last week when the BBC breakfast programme were reporting about children’s use of “skinCARE products”. Apparently popular now with some girls as young as 8. A young girl was interviewed and explained that she loves the packaging and their attractive colours (just as happens with vapes) and was asking relatives to buy the products for her – and they were doing so!
The Dermatologist explained about the dangers of these products for children’s skin, to which the female presenter added that some of the ingredients can affect hormone production and fertility.
The dermatologist dismissed her comment with the words “I’m not so worried about that side of things” and went on to talk about young skin etc. She agreed about the toxicity of these products to youngsters.
If children as young as 8 are damaging their skins with these products, progress to the vapes that also attract them and then end of up on ADs, it’s hardly surprising that fertility problems are the result is it?
Surely dermatologists should be taking the problem of fertility a lot more seriously than appears to be the case. They were very slow to accept the fact that RoAccutane caused so many problems weren’t they. Seems they are no more open to this truth ( if it proves to be so) either.
annie says
However, Anne-Cécile Mailfer, president of Fondation des Femmes (the Women’s Foundation) said “Leave our uteruses in peace,” on X (formerly Twitter).
2023 HCFEA in France reports that an increasing number of French young people are on psychotropic drugs. The response from psychiatry is this shows lots more children need help with SSRI and related drugs.
“A 46-year-old cisgender man with no children comes to give us lessons on how we should use our uteruses,” added campaigner @jeneveuxpasdenfant on Instagram.
https://www.msn.com/en-gb/health/other/france-is-giving-out-fertility-tests-to-women-in-their-twenties-but-not-everyones-happy-about-it/ar-BB1hbUm5
Fuller version
‘Leave our uteruses in peace’: Fury as Macron offers free fertility tests as French birthrates slump
https://www.itv.com/news/2024-01-23/president-macron-offers-free-fertility-tests-as-frances-birthrates-slump
French President Emmanuel Macron has caused controversy with a series of new measures to tackle France’s declining birth rate – including free fertility tests and better paternity leave – in what he described as “demographic rearmament”.
France’s birth rate is at its lowest since the Second World War, with just 678,000 babies born in 2023, according to census data by INSEE. That is a 7% decrease from 2022 and a 20% drop from a peak in 2020.
“France will only be stronger if it revives the birth rate,” President Macron said during a prime-time TV press conference.
“A new, better paid parental leave will allow both parents to be with their children for six months if they want,” he said.
But it was the “major plan to combat infertility” that caused a flurry of responses on social media.
Free fertility check-ups for everybody aged 25 would be introduced, Aurore Bergé, the equality minister, said, while additional funding would be made available for assisted reproductive technology and more research into bodily chemicals that can hinder fertility.
But some critics say the new measures are not the best way to tackle the slumping birth rate.
“Leave our uteruses in peace,” Anne-Cécile Mailfer, president of Fondation des Femmes, the Women’s Foundation, posted on X, formerly known as Twitter, in response to the announcement.
The group advertises itself as the leading French foundation for gender equality and working to eliminate violence against women.
“A 46-year-old cisgender man with no children =comes to give us lessons on how we should use our uteruses,” one feminist social media campaigner, who goes by the username jeneveuxpasdenfant – meaning “I don’t want any children”- wrote on Instagram.
She, along with other critics, attributed an unwillingness to have children to the high cost of living.
This and climate change’s impact on the planet, a societal system that leaves women bearing the majority of the burden when it comes to childcare and some people simply not wanting to have children, have been listed as reasons.
Promoting French values in the face of populism
The birth rate-related proposals came as part of a news conference by President Macron on January 17 in which he answered questions for more than two hours.
“I still have three years and a half in office,” he said, describing an ambition to change the daily life of the French while also tackling global crises.
He detailed how he would preserve France’s struggling health system and accelerate changes at schools.
‘and more research into bodily chemicals that can hinder fertility.’
Sex, Fertility, France and Serotonin Timeline
ouvrir les yeux …
Bernard says
Is there a source for the 6% PSSD prevalence figure?
Dr. David Healy says
There is a paper by Yassie Pirani which she is trying to get published. There are papers by Montoya et al from over a decade ago suggesting no more than 50% of people return to normal sexual function months after stopping. Depends on what you mean by PSSD. There may be tons of people on SSRIs who can’t stop who have PSSD. It seems established that a lot of men with premature ejaculation are helped with an SSRI and many of those remain helped after stopping – that is have delayed ejaculation and orgasm compared with what they had before.
Its beginning to look like – once treated, to some extent changed forever
D
D
Peter Selley says
Thank you for a useful aide-memoir of the long history of this chemical merchandise.
One can also look at the short term history – over one generation – a pregnancy.
Pre-conception – PSSD and defective sperm production could both cause a relative infertility.
Whether suicide rates in pregnancy are higher in mothers taking SSRI’s is not known.
Although poorly studied, antidepressants may affect the physiology of the mother’s pregnancy and harm the placenta leading to smaller babies and premature births.
There are documented effects of SSRIs on fetal development in early pregnancy. This may result in structural lesions “birth defects” and neurodevelopmental disorders.
Worryingly, in female fetuses this is the time that the eggs (ova) are formed in the ovaries. Any damage here may not become evident for 15-40 years if she becomes pregnant.
Babies born to mothers taking anti-depressants may themselves experience severe signs of drug withdrawal during the neonatal period.
Whether children exposed to SSRIs when in utero will be found to have congenital PSSD will have to await an update to the blog post in ten years time.
Dr. David Healy says
You make a very good point about female infertility. Someone needs to be looking out for data on the fertility of women whose mothers were taking SSRIs in pregnancy
D
susanne says
Columbia University Irving Medical Center
OPENMENU
Do Antidepressants Taken During Pregnancy Affect the Fetal Brain?
A conversation with Jonathan Posner, MD, and Jay Gingrich, MD, PhD
News
April 9, 2018
More and more women are taking antidepressants—particularly selective serotonin reuptake inhibitors (SSRIs)—during pregnancy, and many in the field consider this safe. However, some studies, including a new paper published in JAMA Pediatrics by researchers at Columbia University Vagelos College of Physicians and Surgeons, suggest that SSRIs may affect emotional learning, potentially raising the risk of depression later during puberty. We asked the study leaders, Jonathan Posner, MD, and Jay Gingrich, MD, PhD, about the latest research on the risks and benefits of these drugs during pregnancy.
What does the latest research say about the effect of prenatal antidepressant exposure on children?
Posner: The evidence in humans is limited and unclear. A few studies concluded that SSRIs have little or no impact on children. But this may because they didn’t focus on adolescence, when animal data suggest that the effects begin to emerge.
Gingrich: Our mouse studies, dating back to 2004, show that inhibiting the uptake of the neurotransmitter serotonin—which is what SSRIs do—during pregnancy has profound effects on fetal brain circuitry. But we don’t see behavioral changes in these mice right away. In mice, it looks like SSRIs set the stage for increased anxiety and depressive-like behaviors that emerge later in adolescence.
Indeed, we observed this delayed effect in a prior study(link is external and opens in a new window) of health records from more than 15,000 people in Finland. We found that rates of depression in early adolescence were two to three times higher among those who had prenatal exposure to SSRIs compared with those who did not.
What’s happening to their brains that might explain this connection?
Posner: That was the focus of our new study, in which we performed MRIs on infants born to mothers with depression, including those who had been treated with SSRIs and those who had not.
In the infants with prenatal SSRI exposure, we found significant increases in the volume of the amygdala and the insula and increased connectivity between those brain regions.
Gingrich: The amygdala and the insula play a critical role in emotional processing. We see these changes in mice after early-life SSRI exposure and have tied these changes to behavioral abnormalities that appear later in adolescence.
What can you recommend to expectant mothers struggling with depression, and how should these findings be used by their doctors?
Posner: It’s a difficult clinical decision. We know that maternal depression in and of itself can impact the health of the fetus and the relationship between mother and infant. So, doing nothing is not necessarily the answer. But other interventions, such as non-SSRI antidepressants and psychotherapy, can help depressed moms get through pregnancy.
Gingrich: Our mouse studies suggest that the timing of SSRI use matters tremendously. There appears to be less risk in the first and second trimesters. So perhaps you could reduce the dose during the third trimester or switch to a non-SSRI antidepressant. We’ve tested non-SSRI antidepressants in mice and they don’t seem to have any effect on the developing brain.
What needs to be done to get more definitive answers?
Posner: A long-term clinical study, in which we would randomize pregnant women with depression to SSRIs or other therapies and then follow their children through adolescence, would be ideal, but that is not an easy undertaking. Instead, we can engage in a combination of epidemiologic, rodent, primate, and human studies to identify the biological steps leading from prenatal SSRI exposure to depression in adolescence.
It’s critical that we find more answers. Our new findings suggest that SSRIs may be having an effect on offspring, but more research is needed to confirm that. This is not an insignificant problem. Studies show that 8 to 10 percent of women in the U.S. use SSRIs during pregnancy, which means that between 300,000 and 400,000 kids are being exposed to these drugs each year. If we’re doubling or tripling the rate of depression in these children, from 20 to 40 or 60 percent, that’s adding a significant burden of unnecessary depression.financial or other
susanne says
I am adding a comment as some contributors ask about litigation. This research is co-written by a woman in Canada who takes cases on regarding harms from ADs. She may be worth contacting ?
Conclusion from BMJ Open. 2017; 7(1): e013372. Published online 2017 Jan 11. doi: 10.1136/bmjopen-2016-013372
PMCID: PMC5278249PMIn this population-wide cohort study, we found that infants were at an increased risk of cardiac, musculoskeletal, craniofacial, digestive and respiratory defects as well as craniosynostosis from in utero exposure to serotonin inhibitor drugs (SSRI, SNRI and some TCAs). Given that an increasing number of women are diagnosed with depression during pregnancy, these results have direct implications on their clinical management. This is even more important given that the effectiveness of antidepressants during pregnancy for the treatment of the majority of cases of depression (mild to moderate depression) have been shown to be marginal.45 Hence, the need for caution with antidepressant use during pregnancy is warranted and alternative non-drug options should be considered.
Funding: This study was supported by the Canadian Institutes of Health Research (grant number 132750). AB is the recipient of a research chair from the Fonds de la recherche du Québec—Santé (FRQ-S). J-PZ is the recipient of a Quebec-China, postdoctoral fellowships from the Canadian Institutes of Health Research.
Competing interests: AB is a consultant for plaintiffs in litigations involving antidepressants and birth defects. All authors have completed the ICMJE uniform disclosure form.
Ethics approval: The study was approved by the Quebec Data Access Agency and the CHU Sainte-Justine Institutional Review Board (#1740 and #2976).
t here is plenty of research being published via google but most bend over backwards to say it’s not conclusive leaving not only pregnant women at risk but their children too. there is nothing specific in comparison to harms to babies ,even though the publications agree adolescents are more effected with depression if mothers have been prescribed SSRI’s, what the effect is on adolescents’ developing sex lives. Perhaps when youngster who are seen by doctors it should be could be openly asked with mothers’ agreement as her medical history will be a factor which children may not be aware of. As it is youngsters will likely be given more of the drugs which can have higher risks as well as the problems associated with depression lead to inappropriate intervention in the family by social workers and therapists. despite sex being high on the agenda of youngster many will not know what to expect and when to or if to bring the topic up. If the possibility of early recognition was possible maybe some harms could be mitigated before becoming irreversible.
An official website of the United States government Here’s how you know
NIH NLM LogoLog in
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with, the contents by NLM or the National Institutes of Health.
Focus (Am Psychiatr Publ). Fall 2019; 17(4): 372–379. Published online 2019 Nov 6. doi: 10.1176/appi.focus.20190024
PMCID: PMC7011303PMID: 32047384
Clinician Liability in Prescribing Antidepressants
Deborah Giorgi-Guarnieri, M.D., J.D.corresponding author
Author information Copyright and License information PMC Disclaimer
annie says
On this in 2012, with references …
A New Epidemic: Antidepressants During Pregnancy
July 9, 2012 7 Comments
https://davidhealy.org/a-new-epidemic/
Imagine for a moment that a virus started affecting about 5% of all pregnant women—200,000 US pregnancies per year. Imagine that it caused significant pregnancy complications–more than 10% of those infected with the virus would have miscarriage, up to 20% or more would have preterm birth, and 30% of newborns would show effects of the exposure in the days after birth—sometimes severe, with seizures and trouble breathing.
It would be a public health emergency
If this were to occur it would be considered a public health emergency and a tremendous effort would be put forth to address it. Yet this epidemic is happening and, in many ways, it is going unrecognized. Pregnant women and the public are unaware. It is the epidemic of antidepressant drug exposure during pregnancy.
Mr Justin Oxley says
Hopefully it is only 6%, that equates to half a million people in the UK. I’m struggling with nerve pain currently it is worst in the early mornings and has been waking me very early for the last couple of weeks just after midnight. I have managed to taper down to 0.5mg of the liquid Fluoxetine. Perhaps I went a bit too quickly dropping the dose by 0.1mg in January ?
On the plus side I take just one 40mg Propranolol tablet each morning and that seems to keep my BP and pulse at sensible levels.
I still feel pretty lousey during the day and walking around and getting stuff done is hard work and I am really quite clumsy at performing every day tasks in the kitchen etc.
I’m staying at 0.5mg for February as I really don’t need the nerve pain to get any worse.
Mike says
Dr Healy I noticed you made a post on your X (Twitter) January 31st asking people with PSSD in the UK to volunteer for research I liked the post but there’s only 20 likes (currently) I think perhaps you should mention this research on an upcoming blog post because I think the blog is the main part of your website that people view the most. If I wasnt 40 years old and if I lived in the UK I would volunteer.
Gio says
Well… too bad for people like me whose depression and anxiety are unbearable and are forced to stay/return to antidepressants. I honestly don’t know if I suffer from pssd. When I was on antidepressants I could sometimes have sex, and more often not. Same when I stopped. And same when I started suffering from anxiety/depression before taking antidepressants. Anyway I tried to stop taking them as I wanted to see if I could live without them. I am 4 years free but my mental health and general health have deteriorated so much so I am now contemplating the idea of going back on them. My takeaway from this is that if you start suffering from some sort of mood disorder you sre basically fucked because the disorder itself is life altering but the “cure” is not actually a cure. And in these 4 years I tried everything under the sun to try to imprive, from mindfulness/meditation, to dietary changes and sports, to therapy and supplements. Nothing helped. So here I am.
annie says
You could get a million answers to your current dilemma, and it is a dilemma.
In some ways you are the perfect patient. A doctor would unfailingly prescribe you an antidepressant of his choice, as you say you have tried every resource,
He might say you have TRD. He might say lets try a different antidepressant, but what he won’t say is that it is a gamble as to whether you will get severe PSSD, that you might remain permanently hooked, or will endure a complete numbing of your emotions.
Contemplating a return to antidepressants is a right for all of us.
What I worry about most of all, is that you might get yourself back on an antidepressant and when feeling ‘back on track’ want to come off it.
There is the possibility that your current symptoms stem from coming off your antidepressant quite quickly. Anxiety and depression can result from an injury from a too fast withdrawal which can manifest itself a long time later.
Doctors don’t recognise this as a factor, hence the adding of numerous other drugs like Propanolol and Benzodiazepines and off you go on the slippery slope of a poly pharmacy regime which will not help you at all and will make any subsequent diagnosis almost impossible.
People have had horrendous problems trying to get off their SSRI, and if they do eventually get off it are, in the main, too terrified to even contemplate another go. The PSSD people live with their regret at going anywhere near these drugs.
You have a completely understandable dilemma on your hands, and at one time I used to think ‘god, give me back the Seroxat’ as my doctor said, I had ‘incapacitating anxiety’ but did not suffer from ‘endogenous depression’; doctors can be dangerous.
This is when you have to listen to yourself.
There is no magic bullet; but bullets can come when you least expect them.
Addressing ‘unbearable’ symptoms; your contribution is valuable.
Gio says
Thank you very much for your reply. I appreciated it. It is my choice, I know, and I am completely stuck. I came off paroxetine 4 years ago. The doctors told me to come off in 1 month. I did it in 8 months and maybe it was too fast anyway. Then 2 and a half years ago I started feeling worse and worse as i waa also trying to come off benzodiazepines. I couldnt manage to do that. In that period of time i lost everything: my job, my relationship. I still remember the living hell of coming off paroxetine but i cant compare it to howbi feel now. Now i have constant anxiety and physical symptoms but again, i dont know what to do
Anne-Marie says
Gio try this book. Shirley Trickett Coping Successfully with Panic Attacks. It’s a brilliant book and stopped me from having panic attacks caused by anxiety. I have recommended it to others who also found it helped them too. It will help your anxiety by teaching you how to relax with breathing techniques, exercises and healthy eating. It really does work if you follow what she says.