
This post links to From Just Say No to Getting to Yes.
If I prescribe you a medicine, the science starts when you swallow it. The observers at this experiment are you, your family, friends, people you work or live with – and me.
Science is said to be based on Show Me not Trust Me. So you might say first Show me the Evidence – Inform my Consent.
Can Consent be Informed
Informed Consent originally meant telling you that the drug you were about to take was unlicensed – see this 1962 consent form from Louis Lasagna who introduced informed consent to company trials.
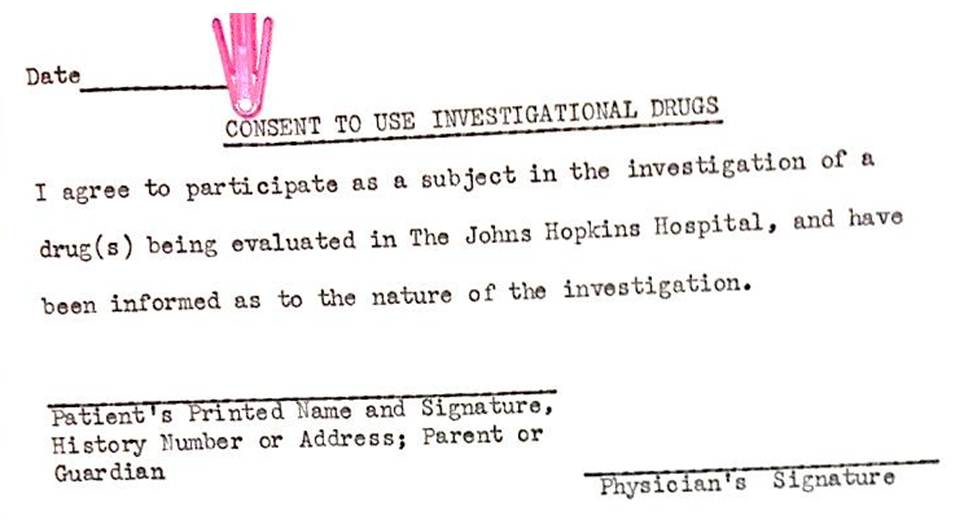
It might sound obvious but No Drug you take has been licensed for you.
Companies then added – we will show your details to no-one else – to the consent form. As a result, the evidence in Evidence Based Medicine (EBM) is Hearsay – like the Bible – it doesn’t meet legal criteria for evidence.
EBM hinges on company claims about their studies, which they call Randomized Controlled Trials (RCTs) and bill RCTs as Gold Standard Evidence. RCTs are designed to inform clinical care but company studies are designed to get a product licensed letting the company market it in a manner aimed at over-riding informed clinical care.
In these licensing studies, you are more likely to die or be disabled on the product than on a placebo. You don’t hear about this because it’s not what company studies test nor the basis on which regulators license products.
Companies make more money if you get hooked to their product in the case of a drug or need yearly shots in the case of vaccines.
The information you swallow, supposedly there to keep you as safe as possible taking a dangerous chemical, is designed primarily to keep the company safe.
Prescribed drugs come with a label written by the company making it, who have simple ways to make injuries, like Augusto’s and Brianne’s in the article above, disappear.
For several decades, companies have ghostwritten the literature on their drugs, often fraudulently to the extent of publishing negative studies as glowingly positive.
NICE and all guidelines (standards of care) have to be based on studies and there are almost no studies on prescribed medicines other than company studies. The companies, therefore, essentially write the guidelines.
Nobody gets to see the study data. Suicidal and homicidal patients who dropped out have been coded as dropping out for nausea or burns or unspecified intercurrent illnesses.
Healthy volunteers given medicines have committed suicide or had other serious problems within hours or days of them starting or stopping a medicine, which companies have assessed as caused by their drug but have neither given the study nor the assessment to regulators.
Are the millions of reports to FDA’s MedWatch and Clinical Case Reports of drug consequences not evidence? For Austin Bradford Hill who created RCTs, and most doctors up till 1991, these reports were Gold Standard Evidence, but doctors now on cue, like a company chorus-line, chime along with anecdotes, misinformation.
The communities of folk gathered on internet collectives injured with conditions like Post-SSRI Sexual Dysfunction (PSSD), many of them PhDs or medical doctors, provide compelling evidence. But Facebook and other social media have been pressured to shut down these ‘breeding grounds for treatment skepticism’.
Promises, Consequences & Statistics
Aren’t journal reviewers and statisticians there to spot problems despite the ink squirted by a company-octopus?
Company studies are worth Billions to journals. Senior figures from Elsevier or Reuters sit on company boards, obliging them to boost company sales. The editors Elsevier hire are not going to get in the way of this by appointing reviewers with a record of trying to peer behind the ink.
The statistics linked to company papers enhance the fairy tale we are sold. The gospels (good news) doctors now read have fairies with magic wands making promises shine and consequences disappear.
So much so that eminent safety experts state under oath in front of Congress that the statistics applied to company studies mean that we can only say a 100 chamber gun is loaded if 95 of the chambers have bullets in them. Psychotic may be a better word than fairy tale. Even worse, companies don’t count the bullets. They effectively say that on a quick glance we saw bullets but didn’t figure there was 95 there.
Regulators don’t argue with this. Companies, not regulators, stand to get sued but they are confident that Birnam Wood will have to move to Dunsinane before any expert will be able to prove, or court accept, that the gun was loaded.
The 95 bullet statistical lunacy is used to make treatment consequences disappear. What about treatment promises?
Like Adam in The Garden, we are all so susceptible to promises, we might want 95 Magic Bullets in a gun before we risk Banishment from Paradise.

Lost in Medication. Based on Adam and Eve painting by Lucas Cranach the Elder in 1526. © Billiam James 2014
Actually saving lives, however, can be so compelling that with far less than 95% alive on Triple Therapy for AIDs and very few on placebo, this was promoted as life-saving. Triple Therapy, however, was discovered by patients, not by companies and not licensed.
The pressure to save lives pushed down the price companies could charge for each drug. leading Goldman Sachs to state – saving lives is not a good business model.
Instead of lives saved company studies aim at, for instance, agreed changes on a Depression Rating Scale. An on average barely better than placebo Rating Scale score allows FDA to license companies to claim this is an antidepressant.
The barely better than placebo score disastrously allows some to claim the effects of these drugs are nothing more than placebo – they are all in your mind. This is like saying the effects of LSD are all in your mind because on a Good Trip Bad Trip Rating Scale the score comes out as average.
The SSRIs are nothing more than placebo claim is made by folk who don’t ‘know’ these drugs in a Biblical sense – folk who’ve not had SSRIs. It plays straight into company hands pitching SSRIs as more like vitamins than LSD. Few people figure vitamins cause serious problems.
According to FDA, Rating Scale scores show less than 20% of SSRI takers have an unequivocal benefit. Another bunch do worse and a bunch sit in the middle with scores overlapping placebo. Those benefitting do so well we get a minimally positive score overall with less than half benefitting and FDA can license the med.
The Yellow Pill Road

Companies put a lot of work in Getting Your Doctor and You to Yes. A promise of salvation with no consequences is dangled in front of you. Like a vampire, the promise casts no shadow (Vampire Medicines).
We get set up as one of the predestined fortunate creating a sense bad things won’t happen us. FDA, reassuringly, are set up as a father figure supporting what companies say. The FDA approved It Works label – works so well that pregnant women who won’t take processed meats or soft cheeses are seduced into eating and drinking meds.

If you swallow the pill, you are certain to be unlucky rather than lucky. Few medicines are Magic Bullets that cure. None of the psychotropic drugs are. They are therapeutic principles, like glasses for eyesight or the plate in my shoulder, which in terms of function was a better bet than letting my shoulder heal naturally.
Your previously normal serotonin system will be abnormal after an SSRI. Only you can tell if you are one of the somewhat lucky 15-20% who get an effect you find useful that warrants the unlucky consequences for 100% of us who will end up with an abnormal serotonin system?
It is close to 100% unlucky for a baby in the womb. An SSRI induced muting of sensory input might help you later in life but in utero, sensory input is a critical driver of brain development. Muting it is not clever.
Pulling Back the Curtain
Your guide in this Underworld is the Wizard behind the curtain. If pulling back the curtain, you get a shock, keep in mind s/he is likely to be a decent soul who would like to keep anyone s/he sees happy and safe.
S/he is unaware that s/he not you consumes company drugs. Every prescription makes the company money whether you take it or not. S/he doesn’t realise she doesn’t have a thought in his/her head not put there by companies. For him/her these meds are all promise and no consequence.
S/he only has consequences if you come back reporting them. It’s unlikely you will but if you do darken the door of a good doctor’s clinic, s/he will turn to the drug label, the literature and the guidelines, maybe A.I, none of which will mention your problem. She is close to forced to conclude your claim you had treatment consequences is wrong. You’ve misinterpreted something or been fed misinformation.
This is like a pilot faced with you claiming a door has blown off the plane, instructing the cabin crew to tie you to your seat and gag you, maybe lock you in the toilet – anything to avoid alarming others. In mental health settings you risk involuntary detention.
Doctors have been pushed into the morally hazardous corner financiers faced in the 2008 crisis who got the sack if they didn’t sell you products they would never buy themselves.
How do you explain to health service managers that it is Evident to both the person you are treating and you that the medicine caused this problem, when all the ‘Science’ says this can’t happen?
Rather than mobilize the resources of the organizations and associations s/he is a member of to keep you and others safe, as she did before 1991, his/her job now is to keep the organization safe from you.
Types of Wizard
Companies also have our medical wizards taped. They (you also need to ) distinguish between them and produce adverts (evidence) tailored for the:

High-Flyers
Doctors who are happy to prescribe you the latest drug and if things don’t go quite right will add other drugs in. They see themselves as heroically fighting a scourge. You’re semi-invisible caught in the middle. Companies like them because they are the first to start the latest drug they know nothing about, willing to throw it into a mix of other drugs and will push the dose up high.
Semi-Shared Decision Makers
Doctors who use meds a lot and will talk to you about what they are doing but with a view to you consenting to what you are being told to do.
Follow the Rulers
Doctors who like to keep to drug labels, the academic literature and guidelines.
Keep it Simples
Doctors who like meds that dissolve in your mouth so you can’t not take them – or medicines that come in one dose per day fits all sizes. If the medicine causes some dependence this might even be a good thing. Vaccines that need to be given yearly are schedulable and pay well.
These profiles were based on drug reps calling to doctors who figured they were being told about the meds and not realising the rep was there to profile the doctor. These days doctors profile themselves by accessing A.I. which remembers their ‘biases’ – see comments on Ground Control To RSV – RSVP.
Back to the Future
Science emerged around 1660. It wasn’t sold as displacing the authority of Religion or Philosophy. It distinguished itself from them. Religion offered answers, either inviting or commanding us to trust in authority, Holy Books and God.
Science asked questions, many of which had been semi-forbidden before.
In the middle between early science and religion, Philosophy flourished as a source of True Enlightenment. From the Ancient Greeks, it put its trust in logic, mathematics, and other algorithmic methods of reaching universal truths that would hold true in all universes and for all time. It’s goal was true and objectively demonstrable knowledge.
In Latin, this true knowledge, was confusingly called Scientia. Scientia was contrasted with our Opinions, which while often based on common sense, were empirical and ephemeral – anecdotal, potentially misinformation.
Philosophy dared us to Think for Ourselves (Sapere Aude) – but in a rules based way.
Science asks us to Observe Together and come to a consensus.
Hemmed in by Science, our ‘philosophical’ desire for objective truths leads many to embrace the bastardized statistical models outlined above,. When it comes to the consequences of drugs, most statistical models have as little applicability as Logic or Geometric Theorems, but maybe because we have settled on 95% objectivity we somehow figure they do.
Real statisticians who have not been sucked into the Apparatus seek a consensus between the models and the Reality – Us.
EBM when it came along was sold as Science explicitly displacing old-fashioned Authority. The Death of Godlike-Doctors replacing the Death of Gods or Popes. EBM is neither Science nor Philosophy. It’s a Religion whose motto is ‘Follow the Science’.
This puts us back in 1660 where the Mission was to develop the kind of knowledge that comes from Consensus. Knowledge that might be semi-misinformation to begin with but which we could refine, with everyone taking any drug contributing. See Who’s Afraid of Science.
The lack of prior Evidence then and now is an incentive to Science not a problem. There is no Evidence to inform you or me before you take the pill. Being a Scientist does not mean Following the Evidence or having scientific training – it means being an Observer at an event. Religions are there to be followed not Science.
Science comes into play when we deal with the consequences of an experiment.
But just as Galileo and other early scientists had to deal with the Church, so we have to deal with what gets called Big Pharma. This is a misnomer. Industry are not very good at making pharmaceuticals we need. They are better at making propaganda. They have achieved the long sought for goal of propaganda – to turn base lies into golden truth – to become invisible as propaganda and pass as Science.
We are dealing with Big Propaganda rather than Big Pharma.
Tackling Big Propaganda
Detail from Lost in Medication. © Billiam James 2014
Accounts of the Birth of Science often feature an apparatus set up to demonstrate observables, aimed at exploring what people saw but misinterpreted through the lens of biblical or other authority.
Observers could bring their varied biases into the room but had to leave all sacred books or other authorities outside. Allowed to adjust the apparatus or repeat the experiment, they were encouraged to reach a consensus.
Science borrowed its rules of evidence from Jury trials, where 12 people with a range of biases were encouraged to come to a verdict based on examinations and cross-examinations taking place in front of them. They could not base their view on Hearsay – reports of things said or done outside the court room.
The objectivity this process generates is not the universality of logic or algorithms that have no link to time, place and context. It is empirical, subject to revision if new observables come to light. It progresses toward a truth of times, places and contexts. It is based on our judgement calls – not on equations or the images the word Science conjures up for many.
Our collective judgements have transformed our world and underpinned triumphs such as inter-planetary travel, mapping the human genome and advancing our abilities to intervene in human suffering.
In contrast to people who game the system to get access to promised benefits, those with treatment linked consequences have no incentive to mislead doctors. They seek help, not enhancement.
It is when treatments go wrong that we need the strong objectivity that comes from attempts to achieve consensus. A scientific consensus must address observables on which the medicine taker often has a privileged position.
What someone who comes to me says rather than some measurement is key. When I take a blood pressure and recommend treatment because it’s a teench high, I strip one figure out of the context that is you. Hundreds of thousands of your figures are likely in balance, even if some vary from a non-existent average. Treatment risks disturbing that balance, which leads to further treatments ad infinitum. What you say or a conversation about how you look are the best way to assess your balance.
How can you engineer these conversations? How do you invite or challenge a doctor to come to a consensus with you?
Reno
Getting conversations going aimed at coming to calls based on a consensus has been RxISK’s mission from the get go. I am due to talk about these things in Reno on October 4th where I’ll be asking the audience to help Us work out how to get the current medical clergy to embrace science.
There are lots of RxISK/DH posts overlapping with this one
- Truth Trust and Health
- Relationship Based Medicine
- Probity Blockers and Trans Medicine
- Fidere Aude
- Better to Die Rxisking It 1
- Better to Die Rxisking It 2
- Challenging My Doctor to Disclose
- Sex and Evidence Based Medicine
- A Call to H*Arms
We don’t need more Calls to H*Arms. If we are to liberate Care and make it personal and scientific again, we need specific D-Day landing plans and tactics that will work on the bunker your doctor is in and for the problem you have.
Science embraces the individuality central to making us an Us.
annie says
Your previously normal serotonin system will be abnormal after an SSRI.
High-Flyers
‘Doctors who are happy to prescribe you the latest drug and if things don’t go quite right will add other drugs in. They see themselves as heroically fighting a scourge. You’re semi-invisible caught in the middle. Companies like them because they are the first to start the latest drug they know nothing about, willing to throw it into a mix of other drugs and will push the dose up high.’
‘ I am due to talk about these things in Reno on October 4th where I’ll be asking the audience to help Us work out how to get the current medical clergy to embrace science.’
This is wonderful, I have always felt that giving lectures is noble, but audience participation is key. David gave a lecture in France, to doctors, and the Q & A, was almost zero, and if I remember correctly, one doctor was quite rude..
Asking, is key. Without Us participation, things are unlikely to move forwards. Someone might come up with something, which we seem to have failed at in the UK.
In Reno, why are doctors abusive to their patients, when the patient is being perfectly civil and telling them what they don’t want to hear..
Homicide Investigation Underway at Burning Man Festival Following Discovery of Man’s Body Near Reno, Nevada
https://hoodline.com/2025/09/homicide-investigation-underway-at-burning-man-festival-following-discovery-of-man-s-body-near-reno-nevada/
Reno has already been primed; with ‘burning man’ and ‘man’s body’ ..
annie says
“The problem is that we as humans are not great at assessing risk.”
“People just jump from suicide”
RFK Jr. links SSRIs and mass shootings. What does science say?
https://www.washingtonpost.com/health/2025/08/29/ssris-mass-shootings-science-rfk/
Where does the idea that SSRIs could be linked to violence come from?
Rebecca Brendel, past president of the American Psychiatric Association and an associate professor of psychiatry at the Harvard Medical School, said low serotonin has been associated with depression, anxiety, mood swings and other negative emotional and behavioral changes — including both with violence toward oneself in the form of self injury and suicide and violence toward others.
SSRIs work by increasing serotonin.
Girgis said the misunderstanding that SSRIs are linked to violence comes from people conflating findings about suicidal ideation and irritability with violence.
“There’s no link with violence. People just jump from suicide to violence. SSRIs most likely decrease violence. But it hasn’t been tested,” he said.
Studies have shown that during the first few days of starting a medication or stopping the medications some patients can experience what doctors call “restlessness” or irritability.
Jonathan Alpert, chair of psychiatry and behavioral sciences at Montefiore Einstein, compares the feeling to how someone might be after “having an extra cup of coffee” or “getting six hours of sleep instead of the seven or eight they need.”
“This makes people very uncomfortable and this is reported as aggression, but it’s really verbal aggression,” he said.
Brendel said black box warnings are really important so that patients are aware of risks and can be properly monitored. But she added that sometimes those labels can create unnecessary fear.
“The problem is that we as humans are not great at assessing risk. When we see those warnings we can sometimes forget that the FDA determined that the medication is safe for use and effective. And we have decades of data showing that SSRIs are both safe and effective,” Brendel said.
People just jump…
Harriet Vogt says
‘The information you swallow, supposedly there to keep you as safe as possible taking a dangerous chemical, is designed primarily to keep the company safe.’
It’s a given that medical information will be ‘dispensed’ increasingly by AI – the NHS ‘Doctor in your pocket’ or Docpox as you quipped – so I’ve been interrogating Grok* about some of the issues you and Peter raise in your latest RSV post – From Just Say No to Getting to Yes.
What occurred to me during this virtual inquisition is that one reason why people swallow the information – in addition to deeply entrenched and naïve beliefs in the religion of EBM – is that they have no idea where the bodies are buried. And therefore no idea of the Big Questions to ask
It got me wondering – would it be an idea to develop a Rxisk Guide to Unburying the safety signals hidden in Big Propaganda? As a simple starter for 10, these are the sort of questions I (layperson, scientific dunce) was asking Grok about RSV vaccinations:
What evidence is there that ….(condition) ….. (drug name) is being marketed to treat or prevent is – more the result of fear-mongering to make money for pharmaceutical companies – versus proven to make significant improvements to the long term health of patients?
Serious adverse effects – such as valproate teratogenicity, post SSRI sexual dysfunction, and antidepressant withdrawal– often take years to emerge into the public domain. They are mostly buried by clinical trial reporting designed primarily to sell pills, not keep patients safe. But there are always early warning safety signals appearing in case reports, social media and from independent drug safety research orgs like https://rxisk.org/. Thinking about … (drug name) what early warning signals have you picked up?
Please can you do a differentiated analysis of the establishment party line on the safety of … (named drug) compared with critical commentary coming from scientists, doctors and harmed patient campaigners who challenge the conventional narrative? What do you glean about risks that I should know that is not in the mainstream news propaganda?
Can you please list for me all the clinical studies that are being publicised about … (named drug) that have been written by individuals with clear conflicts of interest – and/or by ghostwriters employed by the company?
And any that come from truly independent sources?
I also asked some very specific questions like – why are manufacturers lying about seizure risk with Beyfortus? What can you find out about real drug pricing vs hospitalisation costs? In the second year after mass immunisation, the RSV season in Chile is looking disastrous. Here’s a piece from Dr Peter Selley – whom you’ve mentioned. What are your observations on his findings?
I’m sure you can do a far better intellectual scalpel job than me – but it’s a thought. And a start.
One last quite interesting- albeit intuitively obvious – thing I found out from Grok by asking, ‘what sorts of questions are pregnant women asking about the benefits and risks of RSV vaccinations for their newborns? How deeply are they thinking and probing?’ There is inevitably a spectrum from ‘from practical to highly sceptical’. The Big Propaganda ‘market’ segments as follows – making Rxisk patient communications’ targeting and content needs clear:
THE FAITHFUL MAJORITY – relying on trusted sources, e.g. their Ob-Gyn, paed, CDC resources, seeking confirmation rather than challenging the narrative.
Surface level questions: about logistics (e.g, timing, co-administration), accepting CDC or ACOG guidance at face value. Reassured by claims, e.g. Beyfortus 79-90% efficacy, undeterred by ‘mild side effects’. Sounds like your sensible four.
THE SKEPTICS – digging deeper into safety concerns and data, particularly about pre-term birth (5.7 vs 4.7 placebo) or hypertensive disorders with Abrysvo, lack of long term data on Beyfortus.
Often explore alternatives like breastfeeding – question whether RSV severity justifies intervention in healthy infants etc.
THE HERETICS – a less common but growing critical thinking subset. Influenced by vaccine ‘hesitancy’, posts on X (e.g. concerns about clesrovimab’s mortality data). ‘These women probe pharmaceutical motives, citing high costs ($519.75 for Beyfortus) or rapid approvals as evidence of a ‘money making racket’, similar to your earlier sentiment. They ask about whether RSVs hospitalisation risk (1-2%) is overhyped for healthy infants.
*Elon doesn’t need any promotion for his baby but, imo, Grok does have some definite strengths over ChatGPT – it’s real time, linked with X, so relatively uncensored like its owner, giving out both Big Propaganda and critique from those who can still think for themselves – both professionals and patients. I don’t find the fact that it’s chummy sinister- it remembers how you think and speak, which makes communication easy and instinctive.
annie says
Doctor hits conference hard
Dr. John Campbell
“It’s time for everyone to stand up to corporate tyranny”
“Just say no”
https://www.youtube.com/watch?v=mEgAi1TK99o
Dr. Aseem Malhotra talks doctors, regulators, medical journals, with a hard-hitting exposé in 18 minutes flat-out..
Tackling Big Propaganda..
chris says
My sister died 3rd August 2025 we were told from a massive bleed on her brain. She had been on citaloprom for many years and then developed a heart problem and was given apixaban. I tried warn about the drugs while watching her decline but she would demonstrate a slightly patronizing brush off poliety articulated in a very British way which stated the family hierarchy without the words you’re beneath me and not a doctor. Am left to deal with the ongoing grief of my mother.
Dr. David Healy says
C
This is grim. It is hard to believe that medical practice has disintegrated to such an extent. The incentives are badly misaligned. I have a forthcoming lecture in Reno that will deal with this and asks what we can do to put a premium back on safety.
D
chris says
Hope it will be filmed. Of course I meant citalopram.
There is a hopeless feeling when you can’t even persuade a member of your own family they are putting themselves in great danger by continuing with these drugs…you have all the evidence but no way to get it across.
Dr. David Healy says
Yes you are pointing to another key part of the puzzle – our families want to believe in the authorities. You sound like you/we have a modern version of a prophet is not honoured among his/her own people.
The Reno talks – not just mine – Kim Witczak will be there too – will hopefully be recorded and will be up for viewing pretty soon afterwards. Will also have the text on DH
D