
MEDICAL CARE MEDICAL SCIENCE
This talk was given at the request of Professor Ilana Crome to healthcare staff and students linked to the UK’s Midland’s Partnership University on January 12, 2026.
Slide 1: In the US, the term medical model translates to a pharmaceutical, model – a giving meds model. The term medical model began in Paris in 1800 and linked medical disorders, like tuberculosis or raving insanity in folk confined to asylums, to disordered biology rather to the whole person..
For Americans, claiming the suicide, homicide or sexual dysfunction SSRIs can cause validates the medical model does not compute. Or that knowing when not to give drugs rather than dishing them out is a supreme medical virtue. This is a medical model – not a pharmaceutical model – talk.
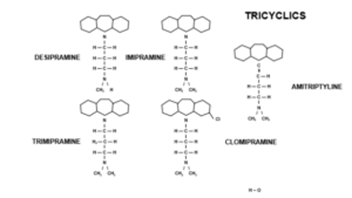
Slide 2. In 1958, Imipramine (in the middle on top) was the first tricyclic antidepressant (TCA). By 1959, European psychiatrists, semi-Freudian mostly, convened at a meeting in the UK, agreed it could replace ECT in the treatment of melancholia. But even in these severely ill, often suicidal, patients, doctors could spot imipramine causing suicide. Doctors today can’t spot SSRIs causing suicidality in mild non-suicidal depressions. Why not?
Frank Ayd discovered Amitriptyline’s benefits in melancholia in 1959, which meant he wouldn’t have to continue giving his father ECT on the kitchen table. Melancholia kills libido and Ayd had no wish to create treatment hesitancy but he could spot and say that amitriptyline caused a sexual dysfunction distinguishable from the effects of melancholia. Doctors can’t now spot SSRIs causing even clearer sexual effects in patients with no prior libido problems. Why not?
In 1961 Julius Axelrod established the 3 drugs on top here all inhibited noradrenaline reuptake, for which he won a Nobel Prize. This gave rise to Schildkraut’s Catecholamine Hypothesis, that the disordered biology in melancholia is low noradrenaline and if we just produce pure noradrenaline reuptake inhibitors, which the tricyclics weren’t, we would have better antidepressants free of side effects.

Slide 2. This was the original low neurotransmitter or chemical imbalance hypothesis. Cartoonists didn’t pay any heed back then because so few people were depressed and taking antidepressants. But 30 years later when SSRIs made depression common, cartoonist spotted the problems with this idea. There were two snags. Benzodiazepines, antipsychotics and stimulants immediately did something clearly helpful. TCAs had lots of effects but apparently no immediate beneficial effect. Noradrenaline reuptake inhibition was immediate but not curative.
Slide 3. This is what melancholia, a disorder of middle or older years, looked like then. After 2 weeks treatment with ECT or TCAs it showed a response. But if there was no immediate beneficial drug effect, what was responding? Did the drugs cure an illness?

Slide 4. Fridolin Sulser’s catecholamine receptor hypothesis replaced the low amine idea. Receptor proteins might need chiseling for two weeks to come right. We now know receptors respond almost instantly but the weeks of chiseling notion legitimized the idea TCAs were curing something. Like the Cheshire Cat, Sulser’s Receptors and then BDNF Biobabble left a Grin behind. We are now told to wait for up to 6 or 8 weeks for something to happen, even in mild problems and we just have to putup with side effects in the meantime.
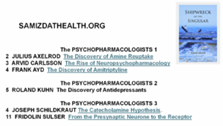
Slide 5. I have over 100 interviews with early psychopharmacologists including Axelrod, Ayd, Kuhn, Schildkraut, Sulser and Carlsson. It costs over $1000 to buy the books these are in, but you can download all interviews for free from the Samizdathealth.org website, linked to Shipwreck of the Singular – See Shipwreck The Psychopharmacologists. Email me if you can’t find them.
Slide 6. In the 1960s some psychoanalysts in both Europe and the US claimed Imipramine, Amitriptyline and Clomipramine had an impact on transference reactions which desipramine didn’t have. The impact was immediate.
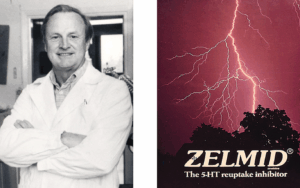
Slide 7. Listening to this, Arvid Carlsson linked these changes in transference reactions to serotonin reuptake inhibition – desipramine doesn’t. He made Zelmid, a serotonin reuptake inhibitor with no noradrenaline effect to explore this further. This and later SSRIs are not anti-melancholic. Changing transference reactions means muting emotional reactivity – their Serenic effect means your analyst finds it harder to provoke you. They are Anxiolytic.

Slide 8. Zelmid was not an anti-melancholic drug but it became an antidepressant even though anxiolysis is where the money is because it was almost impossible at the time for a new anxiolytic to compete with benzodiazepines.

Slide 9. It was obvious 36 years ago that SSRI Marketing needed to shape-shift Valium cases into cases of Prozac, cases of anxiety into depression. Companies platformed doctors claiming depression lay behind many cases of anxiety and treating it would offer a real cure not a drug crutch – besides which antidepressants didn’t cause dependence.

Slide 10: For Carlsson SSRIs were not a Magic Bullet correcting a problem in the serotonin system. Zelmid offered a Therapeutic Principle that allowed us to compensate for a problem. Like LSD, working on a normal serotonin system, SSRIs could cause good and bad trips. Bad enough to cause suicide? Yes.
What’s a Therapeutic Principle? There are 4 kinds of constipation and 4 laxative principles. You can add fluid or bulk, stimulate or relax the gut. The wrong principle for your constipation can make things worse. But a company licensed to use the word Laxative would prefer you to be on 4 laxatives provided one is theirs rather than the right one for you. This way treatment resistant constipation lies.
Most medical problems from hypertension to type 2 diabetes, pain, and nervous problems have several potential therapeutic principles – getting it wrong can create treatment resistance. Euthanasia increasingly is the only way out of SSRI induced treatment resistance.

Slide 11. You might expect Therapeutic Principles for nervous problems to act on the brain, but benzodiazepines relax muscles, and beta-blockers slow heart rates, which fools our brains into thinking we are not anxious.

Slide 12. Therapeutic principles ask us to adjust a function to compensate for a lesion not correct it. Walter Hess, a 1949 Nobel Prize winner, directing his male students to think of functions asked them what their work could reveal about why they fell in love with a girl.
They were all guys back then. The girls were using anticholinergic drops to dilate their pupils which left guys thinking a girl liked them causing them to fall in love with her.

Slide 13. What function do SSRI work on? In 9 out of 10 of us, SSRIs cause genital numbing within 30 minutes of a first pill, at a fraction of the antidepressants dose. The degree of genital numbing correlates closely with reports of reduced emotional reactivity. Reduced sensory reactivity has face validity as a therapeutic principle in nervous disorders – and SSRIs work better for anxiety disorders than for depression and don’t work for melancholia.
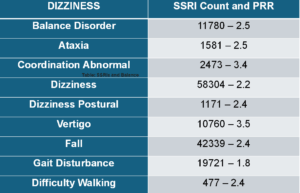
Slide 14. In healthy volunteer trials, dizziness and balance effects are relatively immediate on starting and stopping SSRIs. These are not Side Effects. Balance and touch are sensory effects and are part of the core sensory effects of SSRIs.
This slide shows balance problems reported to FDA on SSRIs. Only 1 in 100 serious problems get reported, so SSRIs have significant effects on our balance for millions of us. PRRs (Proportional Reporting Rates) measure the rate this problem is reported compared to all problems on this drug balanced against the rate this problem is reported on all drugs compared to our drug. A PRR over 1.0 indicates a link, over 2.0 a strong link, and higher again points almost to certainty.
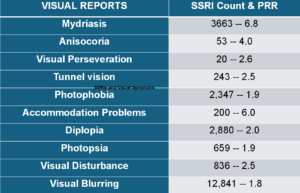
Slide 15. Reports to FDA also show visual issues on SSRIs in hundreds of thousands of us – even though ophthalmologists don’t report them as you’ll hear.

Slide 16. The idea that an action on sensory functions might be Serenic fits with the James-Lange Theory of the Emotions put forward in the 1880s which said our body senses/feels – it thinks fast – what we call emotions are cognitive interpretations/misinterpretations of these feelings.
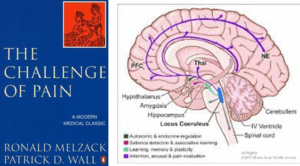
Slide 17. For a century after 1832 when reflexes were first discovered. research established a series of gate controls up through the spinal cord enabling all animals, including us, to function without any mental or spiritual input.
These gates are topped out by a vigilance nucleus – a blue noradrenaline locus coeruleus and the green serotonergic raphe nucleus which damps down vigilance. The locus coeruleus needs our sensory hum to be gate-controlled in order to pick out salient actionable features. The serotonergic Raphe nucleus damps vigilance down. But we can empty out the 5% of serotonin in the Raphe Nucleus, without causing problems.

Slide 18. I am only semi-saying we don’t need brains to work out what SSRIs do. I’m trying to get you to see us as more like Octopi who in contrast to appearances have Distributed Knowledge Centers in their arms – not in the bulbous head.

Slide 19. Acting on serotonin LSD opens our sensory gates, floods awareness, and overwhelms our thinking slow capabilities. The action on serotonin in humans was shown first in our gut. Very early on spiders, who like octopi have Knowledge Centers in their 8 legs and 8 eyes, given LSD wove weird webs.

Slide 20. SSRIs mute these sensory gates. This Brain Scan shows the effects of one dose of an SSRI in healthy volunteers – the sensory input from the body is diminished. Sensory Deprivation Tanks do something similar. This muting might seem to make interpretations easier but in practice muting can compromise our interpretations as you will see.
Slide 21. This quote gives you a sense of how sensorily deprived people can be.
The mental state is literally an altered state of consciousness that one absolutely cannot comprehend if he didn’t experience it. No words can explain such a thing. I am shocked such a state is even possible.
The best way to describe it is mental anesthesia. Everything in the mind is tuned down so low, even thoughts, emotions so muted they are barely relevant.
It’s the opposite of what psychedelics do. They enhance and amplify whereas SSRIs completely mute. One has the impression everything has been wiped out and there is no mind anymore.

Slide 22. Just as Cartoonists knew for decades about chemical biobabble, this Peanuts cartoon shows you Lucy could spot changes in Charlie Brown’s transference reactions as well as any analyst.

Slide 23. Some years ago in this unit we randomized 20 medical and nursing healthy volunteers to a noradrenaline reuptake inhibitor or an SSRI for 2 weeks, then crossed over to the other for 2 weeks. 48 hours into the study a patient asked me if Dr X, who he said was more mellow than usual, was on an SSRI. When we broke the blind – Dr X was on an SSRI and agreed it made him Serene. Patients are expert at observing people in a way healthcare staff no longer are.
The Grin of the Catecholamine Cat inhibits our ability to spot the obvious. Uninhibited patients, cartoonists and psychoanalysts see Good or Bad Trips within hours. Two of our volunteers became dangerously suicidal on the SSRI. Becoming suicidal on an SSRI is not a step on the way to an eventual Good Trip.

Slide 24. One of the main reasons why SSRIs go wrong is that worried SSRIs might not work in antidepressant licensing studies, as this graph shows companies dosed them at the toxic end of the dose range – 20 mg for Prozac. At 20 mg, a range of problems had to be covered with concurrent benzodiazepines. No trials show SSRIs working on their own.
Giving a benzo would not be a problem in a cancer chemotherapy trial because we don’t expect Benzos to be anti-cancer. But using Benzos to damp down agitation in trials of a drug being brought to market to replace hazardous Benzos is perverse.
Looking at this dose response curve. you’d say a 5 mg dose would be optimal. After licensing Lilly published a 5mg Prozac trial. It worked better at a 5 mg dose. It’s lead author Lilly’s Joe Wernicke asked colleagues what do we tell people about this?
Again and again, when someone is not doing well on an SSRI, doctors increase the dose beyond 20 mg rather than lowering it.
Slide 25: Unlike LSD, which we take occasionally and recover from bad trips, we remain on SSRIs for months or years in toxic doses. Unsurprisingly, things break. PSSD (Post-SSRI Sexual Dysfunction), which can last for the rest of your life, points to the profound effects broken sensation can have – see PSSD Podcast .
Bryn: Getting PSSD undermines your faith in the whole system of science as we have it – its not some vague feeling. Losing your libido is equivalent to going blind or deaf, its that level of sensory impairment
Roy: The same can be said for losing your emotions – I felt I lost two senses – my sexuality and my emotions
Bryn: If we want to be believed we have to remember how incredible our story sounds … My Dad says its not possible a drug could cause these effects, it wouldn’t be on the market

Slide 26. A decade ago criteria for a new syndrome Persisting Postural Perceptual Dizziness (PPPD) were put on the map. This dizziness involves vestibular, visual and proprioceptive input – all of which have a serotonergic component. See Balancing our Bodies and our Selves.
Vertigo is a better word for this. For a tightrope walker vertigo would trigger a panic attack and panic is common in people with PPPD. Both starting and stopping an SSRI can cause PPPD and like PSSD or akathisia PPPD can endure for years. Vestibular Rehabilitation Therapy can help but while waiting folk get referred for trauma therapy and get given SSRIs.
This is not just a matter of negotiating things like climbing some steps, we live on a tightrope and our senses manage our subjective balance – disturbances like these strike at our subjectivity.

Slide 27. This fabulous image brings home a key point that disrupting embodied knowledge. as in VSS and PPPD has profound effects beyond just sensory issues. We’ve just published the largest series of cases of VSS linked to one drug group – SSRIs. Like PSSD, PPPD, VSS can start on starting or stopping SSRIs and can endure for years afterwards and people often figure they are going mad – especially with the response they get from health systems.
See Juggling Our Selves and Our Bodies.

Slide 28. Ophthalmologists and others looking into our eyes and not seeing a lesion, tell people this is a mental problem – made easier to say of course if the person is on or has been on an SSRI. They may babble about thalamo-cortical dysrhythmia – a neuro equivalent to chemical imbalance. The patient gets referred for trauma therapy or has an SSRI recommended.
But comparatively speaking there is more serotonin in our eyes relative to their size than there is in our brains.

Slide 29. SSRIs achieve their effects by acting on our primary knowledge generators – our sensory systems. In toxic doses they disrupt embodied knowledge. When this happens, people complain about Brain Fog and are certain their brains are broken but cognitive tests don’t show this.
When embodied knowledge breaks, we try to fix it by attending more which is effortful and frustrating because that’s not the way to repair embodied knowledge – a complaint of Brain Fog proves the point.

Slide 30. Embodied knowledge gets made and repaired by blunt repetition. Trying to instruct bodies doesn’t work. The enduring sensory problems after SSRIs explain why withdrawal is so difficult. There is linked damage that does not go away with tapering.

Slide 31. In 1992, I chaired a UK launch meeting for Sertraline – Zoloft – for Pfizer. I told the audience serotonin was more primitive than estrogens or androgens and drugs acting on it would produce effects never seen before – good and bad. Science is about paying heed to new observations like these – even bad effects can open the door to new drugs.
You also need to know small molecules are promiscuous – they may have 100 effects. If you want precision you need a big, fat protein. Julius Axelrod who rediscovered acetaminophen – paracetamol, often said serotonin was a relic of our marine past. SSRIs act on something even more primitive than serotonin – they activate carbonic anhydrase enzymes – this produces fluid in confined spaces like our eyeballs giving us glaucoma.

Slide 32: This quote from Bruce Springsteen’s Born to Run captures the sensory drivers behind his SSRI linked akathisia.
I was profoundly uncomfortable in my own skin. I just wanted OUT. It feels dangerous and brings plenty of unwanted thoughts. I couldn’t live like this…
I understood what drives people toward the abyss. There was no life here, just an endless irritating existential angst embedded in my bones. It was demanding answers I did not have.
Slide 33. Adding weird new restless sensations to sensory muting opens a door, as this person hints, to having imagery dominate our behavior and to the consequences of that.
Just as my vision lost depth – it was more like a 2-dimensional videogame – there was a loss of depth to my thinking. I was reacting to things on the surface rather than able to see through to the consequences.
If I had an impulse to drive, I would go rather than consider the time or whether I had work the next day. If I had an impulse to go out for a walk, I might simply go without my phone – or shoes
Slide 34. Or this woman who ended up in an essentially hypnotic state.
I was thinking I wanted to stop, that I didn’t want to do it, but I had to.
Why did you have do it?
Because I had started it – I can’t explain it.
When our brains have to interpret weirdly dominant sensations terrible things can happen – its like having command hallucinations.
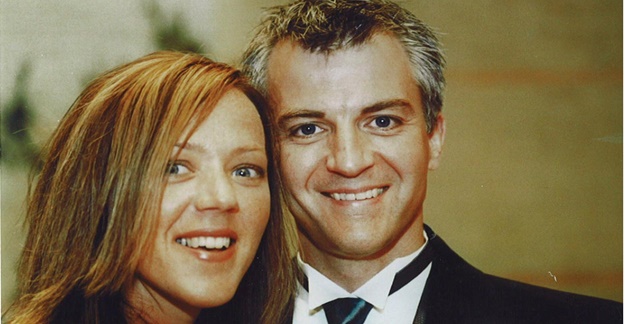
Slide 35. We know SSRIs mute sensation from evidence going on them, coming off them, and from what they break in us. Our right hand knows this. Our left hand doesn’t as you will see from Woody Witczak’s case.
This is Kim and Woody Witczak. He had just begun a dream job, they were happily married, thinking about a family, had booked trips. After a few nights poor sleep, Woody’s doctor gave him Zoloft. He became agitated. One minute he’d be fine, then lying on the floor saying Kim wouldn’t believe the thoughts he was having. Woody had a good doctor who said this was normal – SSRIs may not start working for 6 weeks. Hang in there. In the fifth week Woody hung himself.
If we are dealing with LSD, we don’t say this Bad Trip you are having will any moment flip over into a Good Trip. Why do we say it about SSRI Bad Trips? The Grin of the Catecholamine Cat is partly to blame but there is another perverse source.

Slide 36. I’ve doctored the Great Seal of the United States. E Pluribus Unum – from many individuals, one people – Unum now reads Mediocris – the Latin for Average.
Companies do Randomized Controlled Assays (RCAs) mislabeled as RCTs to get products licensed and claim these offer Gold Standard Science on what their drugs do. They brand Evident PSSD, VSS, PPPD, Suicidality or Homicidality as Anecdotes not Evidence.
Like Chat GPT or Grok, RCAs (even RCTs done by angels) are averaging machines. At best they allow us to say this drug is not totally without benefits, but they tell a doctor nothing about how to treat the person in front of them.
The averaging effect means SSRIs don’t differ much from placebos in the mild depression assays they were tested in. Averaging LSD trials would give the same outcome but no-one says this about LSD. The idea SSRIs are nothing more than placebos kills people.
Less than 50% of SSRI trials were positive but, with adverse SSRI effects damped down with benzodiazepines, a bunch of coding and statistical tricks and some clear fraud, companies could pull out a result that allowed FDA at 6 weeks to license SSRIs as antidepressants.
These licensing linked maneuvers are the basis to the idea SSRIs may take 6 weeks to work. No lesion clears up. There is no evidence in these trials that a Bad SSRI Trip can morph into a Good Trip.
Based on 100,000 patients in company assays, FDA found less than 1 in 6 have a Good Trips on SSRIs. These 1 in 6 Good Trips allowed SSRIs to be licensed as antidepressants.
If companies had sought a license as a Serenic, the trials could have been as short as a week long and would have yielded a marked difference from placebo. Marketing got in the way of this. A Serenic license would have left too much to the discretion of doctors.
Not only do RCTs average good and bad trips on one drug but if LSD, SSRIs, benzodiazepines, stimulants and antipsychotics were all put into trials of mild depressive disorders, although entirely different treatments doing completely different things, they would all end up looking the same – giving the same 3 points difference on a depression rating scale score.
I’m not sure we can blame FDA for this. The drugs have the capacity to work just like they have the capacity to cause suicide. Back in 1990, FDA likely expected doctors to work out how in practice to use these drugs to better effect than company assays suggested.

Slide 37. RCAs allow companies to create a Wonderland. The label attached to their drug acts like the labels Alice faced in Wonderland where food and drink were labeled Eat Me and Drink Me leaving her incapable of not doing this. FDA labels have this effect on sophisticated women who won’t take soft cheeses, or processed meats but consume prescribed SSRIs in ever greater quantities when pregnant.
Freudians who spotted serotonergic impacts on transference reactions can explain what’s going on. Companies have nudged doctors and an educated elite into Delegating Narcissism to FDA .

Slide 38. The Federal Aviation Authority (FAA) licenses planes the way FDA licenses drugs – by looking over paperwork. FAA don’t keep you safe in the air – pilots do. They have an incentive – if you don’t get to New York, they don’t either.
Doctors are health pilots, not FDA. But if the door flies off a healthcare plane and you draw attention to this doctors are incentivized to throw you out through the opening for spreading Treatment Hesitancy.

Slide 39. This is an inevitable consequence of Doctors Delegating Narcissism to bureaucrats. Journalists researching adverse events hear doctors telling them people claiming to know they have PSSD, for instance, have Narcissistic Personality Disorders.
This is the diametric opposite to William Osler’s famous phrase:
“Listen to your patients they are telling you what the problem is”.
When growing up, we Delegate our Narcissism to father figures. In uncertain times we may delegate it to dictators, or gurus. Professionals delegating it to bureaucrats is weird.
Managing Treatment Hesitancy for life-saving treatments is one thing but as Goldman Sachs have told us, making drugs that save lives is a bad business model – the pressure to push down the price of life-saving drugs is huge. Companies make cosmetic or identity disorders to sell profitable drugs, using doctors who they view as devoid of a thought in their heads not put there by them as the front of house sales force.
We are not dealing with a Big Pharma making life-saving drugs, but with Big Propaganda, whose propaganda has become invisible behind EBM and Follow the Science labels, and a chorus line of doctors singing Let’s Do the Narcissistic Tango Again.
If their defenses are challenged, as doctor’s are when someone turns up with very Evident adverse effects, narcissists get aggressive and pick on victims. This system breeds violence. Clinical psychologists seeing the same patients as doctors are mostly too scared to hint that obvious side effects are treatment related for fear of a threatening email or worse from a Medic telling they are not licensed to practice medicine. This isn’t just bad healthcare – it flies in the face of Science.
A note of caution is needed here. I am not talking about Bad People. I am talking about a Bad System. You may need to be as close to the pharmaceutical industry as I’ve been to see how the System works.
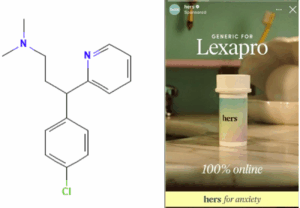
Slide 40. In The Antidepressant Era 30 years ago, I offered a thought experiment. What if these drugs were over the counter (OTC) rather than prescription only. This wasn’t a policy proposal. I was drawing attention to the fact that since 1962, to give you Prozac regulations require me to give you Depression. If I disable you like this, shouldn’t we be sure we can bring good out of this injury?
Switching to OTC bears thinking about as a policy proposal now. The molecule on the left is a potent SSRI but if Woody Witczak had taken it and not Zoloft he would be alive today. Why? Because chlorpheniramine is OTC, and if it didn’t suit Woody, uninhibited by a good doctor, he’d have stopped it. What value do doctors add?
If our drugs work well and are free of problems, we don’t need doctors. Nurses and pharmacists are cheaper prescribers and maybe safer – doctors risk being buried.
In The Antidepressant Era I also said that if these drugs were OTC companies would ensure all of us – not just doctors – wouldn’t have a thought in our heads not put there by them. The use of Tylenol in Pregnancy is a great example of this.
Hims and Hers, and other platforms, now sell prescription drugs OTC – see Authenticity Inc. Telehealth and Influencers. The Creation of Psychopharmacology 25 years ago spelt out how companies like this would ambush us. They use instruments, like rating scales, blood tests or bone scanners, to create figures which their drugs can put right for us.

Slide 41. Checking the figures for our weight began in France in the 1860s. A decade later a new disorder was born – anorexia nervosa. Fasting had been a way to holiness, but became a health and beauty matter. Figures can hypnotize us as easily as icons or incense can.
Companies now create Food Noise scales – See Authenticity Inc – designed to show Glyp-1 agonists muting distracting food noise.
Social Media is full of Apps generating figures, Treating figures gives an appearance of science that hypnotizes us.

Slide 42. Here are rarely seen figures for rates of starting SSRIs among Australian women. The Green line shows figures for women in the 45-54 age bracket who are representative of all older women. The red line shows the rate for 18-24 age group and the blue line is for 10-17 age group. In 1990, antidepressants were rarely prescribed other than to people of middle years but driven by social media they are rapidly becoming drugs for young folk.
See Australian Figures for the Source of these data.
The prevalence of SSRI use for middle aged women is 4 times higher than the incidence figures – breaking up with SSRIs is hard to do – and so prevalence increases with age. The prevalence for the 10-24 age group can never catch up because unlike Peter Pan they do grow up – even so prevalence rates in this age group are rising faster than for any other age – up 110%.
The incidence figures above are for prescribed drugs. How would they look with Hims and Hers online supplies added?
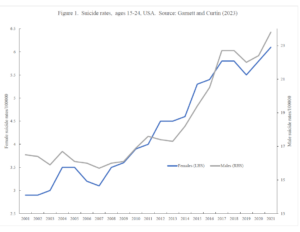
Slide 43. The gray line is for suicide rates among 15-24 year old males over the last decade. The blue line female 15-24 year old rate. See – Damsels in Distress for the source of these figures.
And we now have the first legal cases for suicides after contact with Hims and Hers – Authenticity Inc Meets Grok.
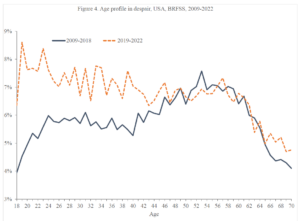
Slide 44. The blue line shows the most solid finding in all of the social sciences – 600 studies showing unhappiness with life is most marked in the 40-60 age bracket and until 2018 least marked in under 24 and over 64s. Links to source data in Damsels in Distress.
But the redline shows a dramatic shift – unhappiness is now most marked among ages 18-40. Are these canaries telling us this mine is about to collapse?
We now have a social welfare crisis with this generation branded Generation Sicknote and talk of countries collapsing beneath the burden of disability payments – See The Great Silence and Damsels in Distress.
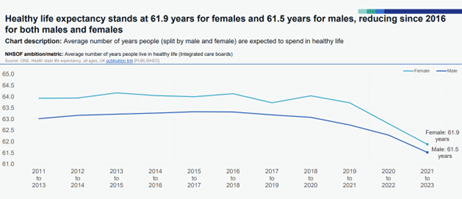
Slide 45: Since 2015 we have also had falling life expectancies and in addition falling health expectancies. The Source is an NHS Integrated Performance Data December 2025.

Slide 46: The small print on the graph above and the NHS Performance Report says we will turn these falling healthy life expectancy data around by focusing on health prevention – which means giving chemicals to healthy people. Doing more of exactly what has caused life expectancy and health expectancy to fall and is bankrupting health systems across the Western world. Lets Do the Time Warp Again.

Slide 47. Science began in London in 1660, when a bunch of men began holding events at which they transfused the blood of a young dog into an old dog and observed – it seemed invigorated. Or looked down a microscope to observe what they called microbes.
These Events produced Observables about which the witnesses, like a jury, were challenged to come to a consensus. Science like a legal trial is an experimental process – it is not something to be followed. It is not a religion – See Health, Care and Science in the Real World.
A Case Report was made for these events and the consensus as to what was happening. No industry or regulators branded these as Anecdotes. This anecdotal process put men on the moon, decoded the human genome and extended life expectancies.
Medical journals came 200 years later. RCTs and their statistics 300 years later. The 1950s was the stellar decade for drug discovery when almost all classes of medicine we have now came into being. None of these breakthroughs involved RCTs. Many of these drugs, like imipramine, which people could see in real life had the capacity to work even if they also had the capacity to cause bad trips, remain better than later treatments. Life expectancies have been falling since the introduction of RCAs – especially in the United States.
There are no observables with an RCT. There are figures but figures are not observables, least of all when processed through statistical models. People are the data and especially with company studies no person can be brought into Court to be examined and cross-examined.
You are not going to hear that this man with an improving Depression score, who dropped out of a Zoloft trial coded as nausea, was in fact Homicidal and Suicidal. Or a man, whose death was coded as burns, was so agitated he poured gasoline on himself and set fire to it intending to commit suicide.
No ‘investigators’ listed on the authorship lines of these ghostwritten (or AI generated) papers can be brought into court to testify because none of them have seen a person given this drug. None of this is Scientific Evidence. It’s Hearsay.
Back when the chemicals we gave were dangerous, Oliver Wendell Holmes famously said:
I firmly believe if all of our medicines were sunk to the bottom of the sea it would be the better for mankind and the worse for the fishes
Our chemicals are still dangerous but today the journal articles, drug labels and guidelines that are supposed to make them as safe as possible to use are even more dangerous. Would he have been forced to say;
I firmly believe if all of our journals, drug labels and Guidelines were sunk to the bottom of the sea it would be the better for mankind and the worse for the fishes
In contrast, every time we prescribe a drug to someone we initiate an experiment that takes place in front of us. We open a door to the purest form of science there is and with SSRIs we have a tool with which to explore some of the most fascinating issues imaginable.
You may say you are in medicine to care for people not to do science – but if you cannot Care if you are not doing Science.
Slide 48. Before engaging in science, this scarecrow, as in The Wizard of Oz, needs a brain, a heart and courage, given to him by an ordinary girl, who may have dilated her pupils to fool him into thinking she can see the courage in him.
He’s supposed to be a professional. That means he puts you and what you need before Church or State, the guideline issuing folk, who want him to get you to conform to what they want you to be.
Rarely in the course of human history have such a small group of people held so much power over the lives of so many as doctors have with prescription-only meds. How have we allowed ourselves to end up in such a weak position as we are in today.
Doing science means having people with different points of view in the room willing to observe and come to a consensus. It means recognizing the person who takes the pill has a privileged position on the observables, as do family and friends.
Becoming suicidal on an SSRI or having other strange experiences on this or other medicines poses a huge challenge to the scientific enterprise – those with a privileged position to observe what is happening will often be understandable wary of telling others much if anything about the thoughts now going through their head, Woody Witczak did not tell Kim that his thoughts included killing her.
Exploring how SSRIs might help needs sophistication – that is an ability to hold contradictory or ambiguous details in mind at the same time and still function.
There are at least 3 steps to better therapeutic outcomes wins with SSRIs.
- Consider micro-dosing SSRIs – dosing to 2-5 mg fluoxetine or less.
- Specify what you want an SSRI to do that might help – name the step on the way to helping. For a beta-blocker we’d say slow your heart rate and ease any shake – not make your anxiety vanish.
- Recognize immediate SSRI effects as their core action not side effects – they are adverse effects at toxic starting doses.
- Support interoception of the sensory changes that enable people to titrate treatment to the right level for them or stop it if need be.
Up the 1980s medicine centered on the problems people brought us. By 1990 we were bringing people into our clinics to screen them for risk factors and essentially were giving them problems they didn’t know they had and putting them on treatments they didn’t need.
When a person brings an ‘adverse event’ to us – this is traditional medicine. They are bringing us real problem and need traditional medical wisdom and relationships.
Good Science is not a matter of knowing research methods and applying for big grants. For a doctor, doing science can pay for itself. You get to trade 100 heartsink patients for 100 free research assistants whose skin in the game is a better qualification for meaningful input than a university degree.
See Pharmacopsychology. Emil Kraepelin would have died for access to an SSRI. SSRIs allow an exploration of our subjectivity, no less. Instead, we have returned to a Dark Age. Never in the history of science have so many observations by so many people been jettisoned by so few.
One reason why the sensory impacts of SSRIs have been ignored is that the sensory nervous system has been seen as too subjective by neurologists, who prefer the reliability of tests for the peripheral motor system and brain scans to variable responses that can change from moment to moment, time of day and time of the month, and can vary by personality type and emotional state. The only tests in common use for the sensory nervous system are biopsies to count the number of nerve endings in skin and even these correlate poorly with what people report.
Catatonia is among the most fascinating subjective mysteries. It lies on the boundary between voluntary and involuntary actions, between assigning responsibility or deciding it doesn’t apply. LSD can trigger catatonia. SSRIs can relieve it.
Hypnosis is another state. SSRIs facilitate it. What does that tell us?
Toxic doses of SSRIs can leave sexual. balance and visual problems in their wake. A genetic variation in PIEZO2 proteins causes sexual, balance and vision problems. PIEZO proteins (1 and 2) are sensory receptors whose existence we stumbled on just over 10 years ago. What other elements of our sensory system are out there waiting to be found? Humility rather than arrogance should be our default mode.
Before SSRIs and Viagra, male impotence or premature ejaculation were viewed as anxiety based needing months or years of damaging therapy dissecting personalities and histories. Lidocaine gel made penises less reactive before SSRIs – what does lidocaine say about the degree of brain involvement in Serenic effects?
How many other states might be helped by a judicious use of drugs to shape behavior rather than correct a disease?
Women disabled by dyspareunia face all kinds of protracted therapies aimed at rooting out their problems. Changing partners can solve dyspareunia (and premature ejaculation). We get told that’s because the new partner is more sensitive. Do we know for sure that’s the case?
In a group of couples, try asking how many women think they could only marry a man with the right smell? Chances are half the women will instantly endorse the idea with others looking flummoxed. What happens when your partner tells you your smell has changed since you began that drug? What happens if she develops parosmia on an SSRI – that might endure for years after stopping?
How much do we know about Material Me or about Material Us?
Note
These earlier posts touch on similar themes:
- Who’s Afraid of Science
- Healthcare Gone Mad
- Probity Blockers and Trans Medicine
- Health Care and Science in Real Life
- Die RxISKing it
- Die RxISKing it 2
The notion of Interoception comes up in the talk. The posts below deal with this and related points in more detail.
- Interoception and Neuroplasticity
- Interoception needs Intrepid Interoceptors
- The Once and Future Pharmacopsychology
- Narcissistic Doctor Disorder
Dr. David Healy says
In fairness to the almost 80 doctors who were at this talk there was 30 minutes of questions after the talk was over.
These ranged from concerns about whether we will be sued some day for prescribing SSRIs – to which my answer is no you won’t. Companies though may well use a threat of being sued – as they once did to get doctors to move from prescribing benzodiazepines to SSRIs.
To questions about what do I do with patients who come in having consulted ChatGPT saying things that may be at odds with NICE guidelines – yes I need to work with patients but I also need to maintain credibility with primary care doctors who make referrals.
One answer here is that NICE guidelines and Chat GPT are likely to overlap considerably – both are based on a ghostwritten company literature. I could show him an email from a previous NICE CEO saying they knew their guidelines are based on a ghostwritten literature but what other option do NICE have – see the davidhealy.org post The NICE before Xmas.
There is an issue here about NICE and Drug Labels gaslighting doctors as much as we the patients figure our doctors are gaslighting us.
To adapt William Osler’s phrase – someone needs to tell regulators and companies – Listen to your Doctors , they are telling you what the problem is.
Another Q was – I’ve used these drugs at much higher doses and never seen a problem.
This is a common point. The question back is whether in some way we aren’t opening a door to hearing about problems. I mentioned that Woody Witczak didn’t tell Kim that one of the thoughts she wouldn’t believe he was having was that he was having thoughts about killing her. Folk may not tell us what is happening because we seem hostile – but it might able be because we seem decent or perhaps even it’s difficult for them to tell us they are thinking about killing us.
There were concerns voiced about the need to get to a minimum effective dose. This is a problem – the so called minimum effective dose such as 20mg of Prozac is in fact a toxic dose.
Another point was helping patients wait through the side effects,
On this issue two things come into play. This was not one of my better lectures in that I was coming down with a dose and the group were listening to me rather than reading this post so maybe the point didn’t come through as clearly as intended.
It’s a difficult concept to get a grip on – that what we are calling the side effects are the core things we want this drug to do. If they are happening in an adverse way it is because we are using a toxic dose.
We want these effects much but in a much milder detectable way that enables the person to work out if this is likely to suit them or not and in a position to work out if the dose needs to be even lower.. They may need time to adjust to the effect and work out ways to make it work for them. .
A recording of the Q and A would have been more interesting than a recording of a poorly performing me giving the main lecture
D
Dr. David Healy says
From Annie
When the Great Forces of Great knowledge and Healthcare and Science Collide
Doctors today can’t spot SSRIs causing suicidality in mild non-suicidal depressions. Why not?
When our brains have to interpret weirdly dominant sensations terrible things can happen – its like having command hallucinations.
Command hallucinations
For Americans, claiming the suicide, homicide or sexual dysfunction SSRIs can cause validates the medical model does not compute. Or that knowing when not to give drugs rather than dishing them out is a supreme medical virtue. This is a medical model
See Kim Witczaks (Un)acceptable collateral damage
https://acceptablecollateraldamage.substack.com/p/guns-mental-health-and-drugs
and it compliments David’s talk, to a T
Slide 23. Becoming suicidal on an SSRI is not a step on the way to an eventual Good Trip.
Slide 30. Trying to instruct bodies doesn’t work.
The more eyes we can open, the more lives we might save. We blindly trusted the system without question, and it cost us everything – Kim Witzcak
Tried and Trusted
Harriet Vogt says
Quite frankly, even if you had been at peak supernova luminosity – as opposed to somewhat off colour – judging by the good doctors’ questions – I doubt if they would have found it easy to grasp what you were saying.
Their knowledge base is disembodied – even ghostly – founded in commercial propaganda. Just taking a quick look at the NICE recommended fluoxetine dosage for adults with ‘major depression’, no wonder mention of a 5mg dose or the contemporary wisdom of micro-dosing seemed to fall on stony ground.
‘Initially 20 mg once daily, daily dose may be administered as a divided dose, increased if necessary up to 60 mg once daily, daily dose may be administered as a divided dose; dose may be increased after 3–4 weeks of initial dose, and at appropriate intervals thereafter.’
https://bnf.nice.org.uk/drugs/fluoxetine/
I’ve been interrogating a few doctors about their education in pharmacology. Rudimentary, my dear Watson. Certainly nothing about SSRIs muting sensory gates, promiscuous small molecules nor far more appealing sounding big fat proteins. I remember Mark H saying, at his prestigious Australian university, they were literally taught – the serotonin deficit theory of ‘depression’. It’s going to take a while to replace that deeply embedded nonsense with the psychopharmacological reality of muting sensory reactivity.
I was thinking of issues that might give doctors a little pause for thought in their quest for a ‘therapeutic dose’ or supporting patients through ‘side effects’ -that are ofc the main action of the drugs.
One reason to think harder is the evidence – also common sense – that the risk of suicide is greatest within the first 28 days. How does this compute with the commercial research artefact of allowing the drugs 6-8 weeks to ‘work’? Doesn’t it make sense to micro-dose and monitor carefully during this high risk period? Better still to see the patient multiple times (as one NHS doctor I know does) until, usually, the misery passes and he doesn’t prescribe at all.
https://pubmed.ncbi.nlm.nih.gov/25693810/
Another pause for thought could be the real world finding you often quote, and emerges yet again in a recent study by antidepressant keenies Cipriani et al – that 2/5 patients dump antidepressants after 8 weeks because they are intolerable – other studies show sexual dysfunction is one of the main intolerables, as well as dizziness. Nothing side about these effects.
https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/realworld-effects-of-antidepressants-for-depressive-disorder-in-primary-care-populationbased-cohort-study/2364972207BAD22AE4A5B30A8BFBB224
I’d heard of the spiders spinning on LSD before, and looked it up. I found one rather amusing quiz in the Washington Post, where you have to match the web to the drug the poor beast was on – including the tears of its enemies, Ovaltine and Charlie Sheen.
https://www.washingtonpost.com/can-you-tell-what-drugs-these-spiders-were-on-by-looking-at-their-webs/e92b3141-7f66-480a-afc6-8290ed88ec13_quiz.html
And a more serious piece of research investigating the effects of fluoxetine on the web building behaviour of Mangora maculate, no less. It seemed significant that fluoxetine ‘increased the web’s radial angle average and frequency of forking and yielded the MOST INCONSISTENT webs.’
Also highly relevant that ‘spiders are unable to build a complete web capable of capturing prey while impacted by psychoactive drugs’.
https://digitalcommons.otterbein.edu/stu_honor/192/
Dr. David Healy says
Rather than reply to Harriet’s great comment, I’m going to lift this response out to stand on its own.
The first point is that the comments from the doctors to the lecture were friendly. They were grappling genuinely with what they had heard even if only half heard because it was so much at odds with the traditional wisdom.
Not only was I off-colour giving the talk, I think I’ve failed to grasp just how much the standard clinical view diverges from what seems to me to be pharmacological reality
The question/insight from one of the doctors that has most stayed with me is the one about having ever better informed patients – who have accessed ChatGPT etc and have plausible ideas about what is happening them but if the doctor takes these on board and agrees with the patient about something that is not in the NICE Guidelines or BNF or drug labels – while many primary care doctors might welcome this some doctor is going to complain about his unprofessional conduct.
Just as patients increasingly claim about being gaslit by their doctors – something that would have been inconceivable 30 years ago – doctors are now being gaslit by NICE, drug labels and regulators. Regulators like FDA often know the literature is fraudulent but its not their job to say so – better to gaslight a doctor than put yourself in the firing line.
As things stand – there is no way for patients to make a difference. They effectively don’t exist. They aren’t the consumers. Doctors are the consumers. And pharma thinks very few doctors have a thought in their heads not put there by pharma (one way or the other).
There might be an occasional doctor who pipsqueaks but until the profession as a group comes around a pipsqueak is unlikely to get anywhere
There will be more about all this in posts to come next week and the week after
D
mary H. says
Recently, I have had two messages, from two people who meet with us for our group zoom meetings. These two messages show the massive differences patients experience when in touch with their GPs.
Firstly, we have a gentleman who has managed to inform his young GP ( a locum I think) of the SNOMED Codes and their usefulness for patients, such as himself, who is no longer taking any psychotropic drugs but remains unwell. He has now managed to get this GP to share all the information that he has given her with the rest of the GPs with whom she works.
The second message came from a young girl who has also come off her psychotropic drugs but is far from well. She asked her GP to give her a SNOMED Code ( I don’t yet know whether or not she used the proforma) and asked for such to be added to her medical record. The GP’s reply was that he wouldn’t be able to do that without contacting the psychiatrist. This he did and the reply ( it seems) which was then given to this patient by her GP was that she must go back on the psychotropic drug if she wishes to have a code added to her record. Obviously, this GP is not up-to-date with his information!
Late in 2025, I met with a young MH Practitioner, who works at a fairly local Medical Centre, who believes in all that most of us here would like far more Healthcare workers to acknowledge. She is trying so hard to convince the GPs there that alternative prescribing ( and deprescribing where necessary) is the way forward. We hope to invite her along to our group at some point as she feels so alone in the good work that she is doing. She is an avid follower of rxisk.com).
Next zoom meeting, we are going to discuss these differences that we come across and try to work out if there is any way that we can make the knowledge, that some seem willing to grasp, acceptable to more doctors. Wish us luck!
annie says
Should we approach this from another angle. If David was a brand ‘Brand Healy’ in a business, he would have a marketing pro like Kim Witczat. Pharmaceutical companies are fantastic at this.
It was quite a feat for David to have 80 doctors in front of him to strut his stuff. A captive audience who clearly were interested or they would not have been there. They should have been sitting comfortably knowing that David is a Medical Doctor. Almost one of them. It is no easy task to cover all the many points that David did. I think his talk contained more points than he has done before, but is there is risk of overwhelming them.
Pretending we are a doctor, for a moment, I wonder what they expected to hear. The questions, as pointed out, were most illuminating.
‘Brand Healy’ has put together the most informative website available Rxisk.org
Wouldn’t we like doctors to use this site. The go-to place where so many questions are answered.
https://rxisk.org/violence-zone/
Videos
Antidepressants and Mass Shootings/Murder Suicide. An interview with Dr. David Healy and Dr. Josef Witt-Doerring
Should doctors be shocked out of their complacency?
And how do you do that without either upsetting them or approaching it like David has done, in a plain speaking, but hard hitting, rational way, which is pleasantly designed to reach out to their better natures.
And then we have the The Maudsley Deprescribing Guidelines to consider.
E S says
I am one of the Psychiatrists that attended the meeting and asked the CHATGPT and GP questions, amongst other comments. It was a very thought-provoking talk.
I think the battle here is between science and regulatory bodies and those that set standards.
The comparison I would like to make is if we were to treat heart attacks or strokes with third of the NICE recommended dose, would we dare to do so without taking an unconventional risk?
If in my practice I start using very small doses and patients are not improving for one reason or the other, although that could be normal even if the patient was to take the current given recommendations, the finger will be pointing at me as a psychiatrist not adhering to nice guidance. We do need some support or backing of a higher regulatory body, and this debate needs to happen also definitely at higher level.
I hope that makes sense.
Dr. David Healy says
Thanks for this comment. This clash is very important. The question is how do we resolve it? There was something similar with thiazide diuretics decades ago – it took several decades to find that they were just as effective at a fraction of the dose.
I suspect this happens a lot with antihypertensives and hypoglycemics where when the patient fails to respond we push the dose up rather than switching this therapeutic principle for a different therapeutic principle.
This didn’t happen so much with benzodiazepines which came on the market without controlled trials – the RCTs set the licensed dose. Clinicians arrived at the doses. Clinicians also made a mistake though with antipsychotics. We got it right with TCAs – we don’t usually go much beyond 150 mg – we certainly don’t use 600 mg which would be the equivalent of Prozac 80 mg.
The antipsychotics are interesting. Low dose haloperidol and risperidone work well – push the dose up and everyone gets akathisia – push the dose of haloperidol up to 80 mg though and the akathisia stops – it seems an adrenergic action gets added in at that dose.
Sometimes we justify high doses on the basis that the psychotic brain is different to the healthy volunteer brain – but its not. When healthy volunteers became suicidal and committed suicide on SSRIs companies said this won’t happen depressed people because the depressed brain is different. But the details of healthy volunteer trials are never published – perhaps that’s one thing that we could campaign for
D
Peter Selley says
This is complex
If you prescribe antidepressants and they commit suicide you will feel “at least I tried”
If you dont prescribe and they commit suicide you will feel bad
If you are youngish, have a mortgage, and live in the area where you work, the pressure to comply is enormous.
If you are out of line with your colleagues it will be difficult.
There are doctors – usually retired – who will stick their necks out to support you.
More evidence is steadily accumulating on the harms of medicines and the harms of too many medicines but this is not reflected in changes in clinical practice.
Prescribers usually follow the guidelines: “if you prescribe ADs, review the patient within 2 weeks”.
There ought to be another guideline: “Don’t prescribe AND review in 2 weeks”
There is some good news
https://www.england.nhs.uk/learning-disabilities/improving-health/stomp-stamp/
People with a learning disability are thought to be 16 times more likely and autistic people 7 times more likely to be prescribed an antipsychotic than the general population.
The NHS lists harmful side effects to them of psychotropic inc antidepressant medications
sedation
weight gain
dyslipidaemia
increased diabetic risk
movement disorder such as extra-pyramidal side effects (EPSE)
hormonal change such as hyperprolactinaemia
ECG changes
sexual dysfunction
and offers help to recognise and deprescribe
It is illogical not to include neurotypical and normal intellect people in this campaign.
annie says
Great Comment, Peter
There ought to be another guideline: “Don’t prescribe AND review in 2 weeks”
I had a couple of friends early in early 2000s, who were around when the whole, horrendous Seroxat took me over…They developed serious problems in their relationship and headed towards a very nasty divorce. The husband told me of the ‘problems’ and rushed off to see our doctor asking for an antidepressant. He came back and said the doctor refused to give him a prescription and to come back in two weeks if he wasn’t feeling any better. He didn’t go back as he got a grip and started to organise his life facing up to it all.
I remember thinking very clearly, so I went through all that with Seroxat, witnessed and promulgated by the doctors, and yet a man with problems causing him havoc, was denied his antidepressant. Well, lucky him. In this instance the doctor saw sense with him, but not with me. I found this stunning in our little rural practice…
Very sage suggestion, Peter
Dr. David Healy says
Capitalizing the AND has a stop you in your tracks effect. A what’s going on impact. There is a lingering – have I read that right.
This might be a tactic that could work especially when the coin drops for people – besides the tactic aspect, the advice is clearly spot on
D
chris says
‘the finger will be pointing at me as a psychiatrist not adhering to nice guidance. ‘
My experience of Psychiatrists is that in front of a patient in a closed culture they don’t give a damn about anything other than pumping them full of drugs. They don’t care if the state you are on is because of what they or their colleagues did prior by prescribing drugs that they reacted to.
One perceptive question was asked of a psych in an on going Inquiry about identifying the difference between a drug induced psychosis and I guess non drug induced and how to treat the patient. A great question which needs intense thinking about.
The psychs reply to this was ‘we treat the psychosis.’ They’re didn’t seem to realise the magnitude of importance to the patient of the question. And there has been no sign that I have seen the Inquiry understands it either.
When I told a psych that he might kill me by his intended action to give me 400mg quitiapine.
His reply was: “Only God knows when you will die.
On akathisia from March last year this was part of a reply to me from NICE:
We understand the importance of this issue, however, we are unable to investigate or intervene in complaints about healthcare or concerns for individual NHS trusts, doctors, or services (including where NICE guidance is not followed) as this is not part of our role.
Followed by
“A healthcare professional would be expected to refer to appropriate guidance when prescribing medication. They would need to consider and weight up the potential risks and benefits of a treatment on a case by case basis, in discussion with the individual, before deciding whether it is an appropriate treatment for them.”
“As you are aware, NICE are not asked to develop guidance on all conditions and our recommendations do not cover all clinical circumstances. We have not published any specific guidance on akathisia.”
Dr. David Healy says
Chris
This is a great comment and I’ve definitely heard the things being said you’ve heard – got told. We can all fool ourselves but the doctors on this call seemed very decent folk to me and the tone of voice and body language with the questions all felt genuine to me.
I think though there is an important issue here – the sign of a good doctor has become adherence to NICE guidelines and the evidence base. There is a real logical bind to doing something that is not evidently evidence-based. Even if I’m confident that I might be able to defend my actions – the inquisitors are not going to easily accept that the evidence endorsed by NICE etc is junk – does not meet legal standards for evidence.
The problem we have is like the problem women face in a patriarchal society – where the legal systems etc has been set up by men who have never been sexually assaulted or raped and can’t understand why asking a woman for details of the assault which she may not be able to recall clearly is not the way to go. Where putting the woman who is the victim in the witness box and interrogating here as though she were the criminal trying to get this poor innocent man convicted for some perverse female reason
Even good men risk getting sucked into a system that casually damages women. I’ve heard close friends defend male colleagues guilty of shocking abuse – like Gideon Koren – they see someone whom they know as Decent as a Good Sort. The entire University of Toronto system – a very male hierarchy – mobilized around Koren to protect him from a woman – Nancy Olivieri – who they portrayed as someone more concerned about whether she had the right hairdo for her portrayal by the latest media.
Harriet’s point about all the doctors who’ve been SSRI assaulted is a good one – is there anyone in there or among RxISK readers who could write a play like Prima Facie. I’ll hopefully be able to get round to writing something more on these lines in the next week or two
D
Harriet Vogt says
A pertinent post on X today by Sam Hall who moderates one of the largest online withdrawal support groups, educated by his own grim and ongoing experience (that he has made public). A fast taper off sertraline after 13 years, yet agqin withdrawal misdiagnosed as a ‘mood disorder’, switched through 11 different psychotropics at speed – oh, and labelled with FND, as a final insult.
As of December 2025, 1,244,238 individuals belonged to online support groups dedicated to tapering psychiatric medications and withdrawal support.
·
‘Importantly, many of these groups include psychiatrists, GPs, nurses and allied health professionals, often seeking guidance to taper the same drugs they prescribe, after encountering similar barriers within the healthcare system’.
https://x.com/samhall404/status/2011787438859952308?s=20
Not only are doctors finding themselves conflicted by commerically driven guidance at odds with patient experience and real world wisdom, but some are so gaslit by their own professional guidance they are defecting to citizen scientist peer support .
What I’d say to Dr ES – whose professional dilemma is entirely understandable – there seem to be growing numbers of doctors questioning the guidance that corrals them, especially those who have been harmed by it. It is time for the converts in the profession to stand up en masse and be counted. There are some at NHSE – who are listening – at least for as long as NHSE exists. There appear to be others in the US system (which also penalises the poor) – I noted that Adam Urato has been appointed to the advsory Committee on Immunisation Practices.
As a mere mortal not medic , I find it extraordinary that doctors wouldn’t see something fundamentally amiss with a class of drugs , SSRIs, that interfere with the sexuality of between 25-73% of their patients? This is a drug effect, not a misery effect? Hardly a desirable serenic efffect either. Wouldn’t common sense suggest reducing the dose?
https://www.dovepress.com/antidepressant-associated-sexual-dysfunction-impact-effects-and-treatm-peer-reviewed-fulltext-article-DHPS
And what about anti-psychotic induced parkinsonism – estimated I believe to afflict about half of all patients over 60 years on long term AP ‘treatment’? Dose reduction is recommended – of course it is.
I know the family of a 20-something patient who went a bit otherworldly in protracted rx topical steroid withdrawal – as you would, if your skin was suppurating for several years. The patient was diagnosed as ‘schizo-affective’, suppuration was ignored. Drugged out of mind and body on max dose sertraline (no clinical rationale) and questiapine – leading to obvious AP induced parksinsonism, urinary incontinence, a dropped neck and zombification. Sick of this, the patient went cold turkey off both medications. They are certainly suffering from physical withdrawal – nausea, bladder and bowel issues, stiff gait, tics etc. – but there is no sign of the ‘psychiatric relapse’ that has been the primary clinical concern. This stems from adhering to guidance and non-existent average patient number crunching. As David often says, it is the individul patient who is doing the science. And patients have spent decades campaiging and trying to educate a blinkered, defensive system.
Dr. David Healy says
There were two more questions/comments that have come back to me.
One was from a colleague working in CAMHS – children and adolescent mental health services who said they always start low but do aim to get up to the minimum effective dose. The problem with the so called minimum effective dose is that in the case of SSRIs or SNRIS (same thing as SSRIs) it’s nothing of the sort. Its a toxic dose.
She also said they have a lot of autistic spectrum disorder (ASD) referrals. Part of the problem here is ASD likely in many cases simply means introverted teens. But because autistic has replaced introverted, there is an assumption these teens may not be able to interocept. For most of these patients this assumption is just not going to be right.
There was also a hint that SSRIs can dysregulate these folk which seems more likely to be a case of SSRI dysregulation/ disinhibition – as can happen with healthy volunteers young or old and is a drug effect that has nothing to do with an autistic state.
The paradox to some extent is that the most common neurotransmitter theory of autism is that it has involved high serotonin levels – the opposite imbalance to what is claimed for mood disorders.
D.
Dr. David Healy says
Professor Ilana Crome who organized the meeting works in addiction medicine. She was struck by several things. One was the idea of microdosing SSRIs and she wondered if the turn to microdosing psychedelics might open a door to making this possible with SSRIs also.
Another point was the research on psychedelics builds therapists and therapy into the treatment package. Would this open the door to more joined up working with antidepressants?
The trouble with therapy and psychedelics is that at present the therapists know little about what the drug effects are and they risk misinterpreting things.
On psychedelics do we actually meet God or see the afterlife? How does this marry up with the physical states that bring us close to death and give us similar experiences? And if someone from new york passes through a tunnel to the afterlife it is often a tall building tunnel whereas someone living rurally won’t have tall buildings – why not?
Ilana’s sense was no one mental health is getting much training in pharmacology.
D
Anne-Marie says
Kevin Roy on X said this below. Ssris really do act like dental anesthesia on everything.
SSRI impair perceptual depth. Without depth we can’t assign meaning. Without meaning we can’t assign emotional value.
When you alter the function of the nervous system with a drug you will change how the world is perceived and therefore change the meaning and emotional value.
If you prevent communication with the effects of lidocaine commonly known as freezing in dental work. Immediately those tissue’s loose meaning and therefore the emotional value is not perceived. Allowing the dentist to work on your teeth pain free.
The SSRI is not different than lidocaine of having an anaesthesia effect. They both remove meaning. Hence the SSRI reduces emotional value thereby making the depressed undepressed.
Dr. David Healy says
That’s a good way to bring out the point – thanks for passing the comment on – but who is Kevin Roy?
D
Anne-Marie says
He’s on X and was on ssris himself. He explains the side effects and his experience very well.
Dr. David Healy says
Giving good descriptions of the experience is important and useful. Most explanations of the side effects are likely to be a mixture of biobabble and more biobabble
D
Anne-Marie says
I like his explanation because he deep dives into each side effect explaining it with more depth. I know I don’t explain my side effects enough because I don’t know how to explain it. He does this perfectly. I like that he points this out like critical thinking is effected for example by emotional numbness and detachment. This lack of critical thinking can cause all sorts of problems in daily life and relationships. It’s very subtle but it’s there and can cause huge problems for people. You look at research papers on emotional blunting and detachment and all you get is how it creates more positive thinking and perception but in reality you need negative thinking as well for critical thinking. You lose negative thinking when it’s just as important to have as positive thinking.
Noone talks about how important negative thinking is when it comes to critical thinking. This is just an example but this guy explains it in fine detail. This is what I like about his explanations. He says it how it really is. This is very crucial to recognise.
Dr. David Healy says
What you quoted about lidocaine numbing gums and this is an emotional change works for me.
Saying negative thinking is important becomes a bit abstract – more abstract than the quotes in the Are Healthcare and Science Compatible and I Come to Praise SSRIs not to Bury Them where a person on one of these drugs says his vision became 2-dimensional like in a videogame – he couldn’t see below the surface to the consequences and the same applied to his thinking so he was doing things much more on impulse. This is much less abstract.
But Kevin Roy also chucks in a load of dopamine GABA and SSRI biobabble that for me anyway drains everything else he might say of color and meaning
D
Anne-Marie says
I wasn’t interested in his scientific explanation but his explanation of how it affected him interested me because he explains it so well and I can relate to his explanations of his side effects.
I also relate to the guy in the video games you mention.