
Yesterday, the BBC reported that following inquests where older drivers with compromised eyesight have killed pedestrians, and what, possibly thanks to the work of the BBC’s Hazel Martin (SSRIs and Alcohol), the British government has called “a catastrophic rise” in deaths linked to alcohol, it has been announced that there will be a tightening of regulations for eye-testing over the age of 70 and a lowering of drink driving limits – Over-70s face driving ban for failing eye tests
Yesterdays BBC also reported an Australian man’s death after being hit by an over the alcohol limit e-scooter driver – British backpacker pleads guilty to killing man while drunk on e-scooter
Will any of this get to grips with what we can all agree are a growing set of problems? Could the inquests or pending Australian e-scooter court case have missed any tricks?
I’d Like To Tell My Story
This line comes from Leonard Cohen’s A Bunch of Lonesome Heroes.
Several years ago in my forties I was put on sertraline. The background was an episode of depression in my teenage years for which I was given an antidepressant, but there were no further episodes, and the antidepressant had been stopped 25 years previously.
I did well in university and ended up in a creative job that involved some social drinking as part of the business, occasionally heavy, which I was aware of and worried about. I had a seizure several days after a heavy drinking bout. This was investigated thoroughly, and I was told I was not epileptic but I had a low seizure threshold. A link to alcohol was dismissed.
Years later I may have made a mistake taking on the challenge of moving from a secure job to much the same job in a riskier setting, and this led to a prescription of sertraline 100mg, which I was told would be more effective and safer than most of those older drugs.
The information that came with my sertraline made it look good.
At the time I was teetotal, keen to ensure the new job worked out well. I am someone for whom boundaries and focus have always been important. It took hard work to get to where I’d got – there was no silver spoon in my mouth. The new job meant it was possible to work from home a good deal and having my family around helped my boundary setting.
Covid and lockdowns also came along and helped keep me anyway on the straight and narrow, although a year later, I began drinking when the family were away. This slowly extended. I began losing my boundaries. My drinking crept into family time. My work focus began to weaken, and I lost my job.
I increased my sertraline from 100mg to 200mg. Within a few weeks I noticed two new problems. One was with my vision. I could no longer focus on a computer screen without reading glasses. I rapidly moved from no need for glasses to 3.5 strength readers.
The other problem was with my balance. I’m fit. I run and work out in the gym. Balance had never been an issue. But now I could trip even walking up steps if I didn’t pay heed. Preventing myself from falling over required much more attention, more cognitive input than before.
Then a few days after another session of heavy drinking, I had a sequence of several seizures in a row – at home and then in the ambulance en route to the hospital. I know seizures can come with alcohol withdrawal, but I had no other features of alcohol withdrawal at the time.
The investigations the hospital undertook revealed a small amount of brain demyelination. They told me they did not think this was multiple sclerosis.
There were other changes. One day I was standing at a restaurant looking at the menu with a relative, having a normal conversation when I dropped to the ground. I had had several drinks, but this was not a seizure. It happened more than once. In a strange way it seemed as though I had become drunk without being aware of it until I blacked out. There were no hints of the kind of changes that normally tell us we have more and more alcohol on board. If you asked me was I drunk or the relative who was with me, the answer would be no.
The relative with me outside the restaurant later told me: “I think this is linked to your sertraline. There are posts on the web of people whose drinking gets out of control on sertraline.” This relative has no medical training or background in healthcare.
Four years after starting sertraline, I stopped it.
My problematic alcohol intake stopped. There have been no seizures or blackouts since. Over a short period of time my need for reading glasses reduced from 3.5 to 1.0. My balance improved. Recent brain scans show that the area of demyelination has shrunk.
I am not saying that sertraline alone caused my alcohol use disorder. I think I drank more than I should before starting it, but it definitely got worse on sertraline. I do not think I craved alcohol, but I lost my boundaries. Once I started to drink it was difficult to stop and there were no signs of drunkenness to inhibit me continuing nor any care for the consequences.
Leonard’s Heroes
Leonard didn’t know much about Sertraline’s story before he told his story. The original licensing of sertraline was held up by concerns it can cause seizures. Regulators have since had lots of reports from doctors linking sertraline to seizures and convulsions.
He didn’t know that sertraline and other SSRIs can cause osmotic demyelination. See Could your Antidepressants Cause Dementia. This likely happens following disturbances to our water-sodium balance. A fall in sodium levels can be dangerous. When first reported, doctors rushed to replace our sodium rapidly and in doing so they triggered osmotic demyelination. Something similar can happen when we drink. Leonard fortunately caught this early at what looks like a reversible stage.
There are also vision and balance problems. The Tables below come from RxISK.org’s Drug Search tool, which can give us counts for the number of reports specific to sertraline and also for all SSRI/SNRIs.
The counts also allow us to calculate the Proportional Reporting Rates and other disproportionality metrics for any events. Any PRR value greater than 1.0 points to a link to the drug. Any value greater than 2.0 points to a substantial link. The values below all have confidence intervals that confirm them as likely the correct or close to correct value.
The two problems Leonard reported besides alcohol and seizures were vision and balance problems.
Sertraline and Vision
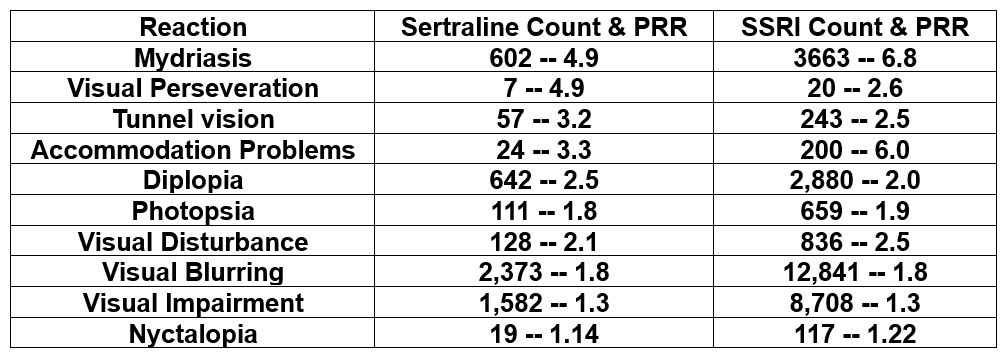
While on sertraline Leonard had accommodation and focusing difficulties one explanation for which may be linked to a paralysis of his mydriasis reflex. Just the opposite to opioids his pupils were likely not constricting – for some of us on sertraline, there may be almost no iris visible. The problem can be worse at night when the lights of cars become more blinding than usual.
Accommodation and focussing problems may be reported to regulators, or coded by them, under a varied set of heading such as mydriasis, accommodation problems or under a series of other headings as listed in this table.
The problem can get worse at night or in low light and lead to dangerous driving even if our pupils are okay. People with Visual Snow Syndrome (VSS) typically have nyctalopia, also called night blindness. Nyctalopia is a more complex condition than mydriasis. It appears linked to a set of cells called bipolar cells, which lie in the retina and have a serotonergic input. See Vision Weird, Vision Blurred, Visual Snow.
SSRIs are among the most common treatments reported to regulators as causing these visual problems.
These findings are clearly significant for the BBC reports above – both in older folk in respect of their vision, younger folk on e-scooters and all the rest of us taking SSRIs.
Sertraline and Balance

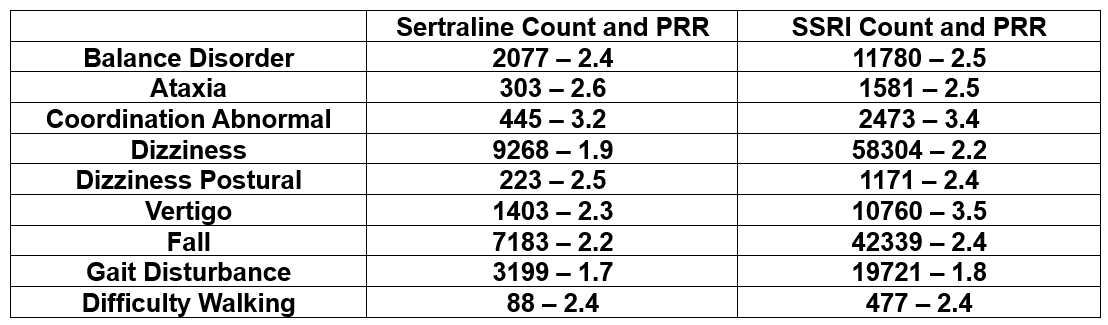
Dizziness is among the most common problems reported on SSRI medicines both starting and stopping. This might sound like a mild problem until you take the alternate headings under which the problem may be reported into account – vertigo, ataxia, balance disorder.
Balance problems lead to falls and disturbances of gait which can be very serious. But unlike vision problems above, which are reflex behaviours, they can be managed to some extent with a cognitive effort and extra attention.
Our visual systems can help us compensate – unless of course they too are compromised. Visual systems typically are also compromised. Balance is complex. It needs input from proprioceptor receptors in our muscles, joints and bones, from the vestibules of our inner ears, as well as our eyes – all of which have serotonergic input.
Losing our balance can give us debilitating panic attacks – for which we will be told the best treatment is an SSRI. See:
- Persistent Postural Perceptual Dizziness – PPPD
- Balancing our Bodies and our Selves
- Juggling our Selves and our Bodies
Sertraline and Alcohol
The vision and balance problems and how these might affect driving were all reported in a 1983 healthy volunteer study that Pfizer ran, from which they concluded Sertraline can cause all these problems. But no regulators or medical journals or anyone got to see or hear about this over 40-year old study.
Tricky and problematic as these visual and balance difficulties can be and were for him, Leonard’s undoing lay in a sertraline induced alcohol use disorder. He is likely right, when he says he got used to drinking more than he should before Sertraline, but he gives very clear descriptions of a change in both the character and quantity of his drinking after he started and while on Sertraline.
Legal systems in general and Governments don’t understand what is going on here or how to manage the situation that a Lunch of Lonesome Heroes like Leonard have taught us – that:
- Sertraline can cause Alcohol Use Disorder
- Canadian Guidelines advise stopping SSRIs if used in alcohol use disorders and not starting SSRIs if there is any hint of an alcohol use disorder – A Medical Triumph SSRIs and Alcohol.
- Alcohol can relieve the agitation/akathisia sertraline causes and this is a potent trigger to drinking – Antidepressant Dysregulation.
- Sertraline can cause a doubling of blood alcohol levels beyond normal – Every Drink Spiked – an Australian discovery.
- These elevated alcohol levels can remain elevated for extended periods beyond normal
Above all Leonard comes very close to the reporting that others on an SSRIs offer about the lead up to events that can turn out to have even more catastrophic consequences than his:
I was thinking I wanted to stop, that I didn’t want to do it, but I had to. Asked why did you have to the answer will often be: Because I had started it – I can’t explain it.
This is close to the heart of what SSRIs do. They inhibit the sensations, feelings, that in Leonard’s case might have alerted him to the fact he was getting drunk.
SSRIs have minimal effects on the brain. They act on sensory receptors in our body to mute sensory input – just the opposite to LSD which opens the gates to sensory input. The most obvious and immediate effect of SSRIs like sertraline is to cause genital numbness within 30 minutes of a first pill at very low doses compared to the doses used clinically.
The same happens to touch around our bodies which we describe not as muted touch but as emotional numbness – by which we mean our feelings are numbed.
On SSRIs many report not getting drunk or being aware of the signs of being affected by alcohol until they blackout. If told the following day they were drunk the night before, they will often deny it.
The many people who have Post-SSRI Sexual Dysfunction (PSSD), which involves a genital and sensory numbness enduring long after treatment stops, similarly report a sense of not getting drunk when they take alcohol that was not there before they began the treatment.
Justice
These are problems for a Ministry of Justice and legal systems. A reduction in sensory input leads to reduced imagery and the action reflexes linked to imagery that we call emotions or sometimes hunches or what Daniel Kahneman called Fast Thinking.
Overwhelm our sensory input by taking LSD and we can have significant problems. Restrict the input, as in a sensory deprivation tank or with an SSRI and we can one image coming to dominate.
If one image dominates it eliminates the free will, and choice, and Slow Thinking that is called into play when we have competing sensory inputs and emotions. Instead, we can end up with automatic behaviour and only come back to ourselves when the trance is broken.
There are profound issues here for justice systems to deal with.
On a more mundane level, what about the millions of us who are driving with compromised eyesight, especially at night, whose problems might not be picked up on optometry screening done by day. What about those of, increasingly young and riding e-scooters, who can’t focus on road or pavement signs properly?
What about blood alcohol levels over the legal limit in someone who does not feel remotely drunk and may be driving competently, who is on an SSRI.
Is it really justice to ban them from driving when the labels of SSRIs don’t give anyone any hint this could happen?
Everything we know about the treatment related effects in this post has come from people like Anne-Marie, Leonard and other Lonesome Heroes – left abandoned by those who give the orders to struggle beneath an extraordinary load.
Leonard Cohen’s heroes were struggling beneath an ordinary load. This sounds like the kind of ‘wisdom’ I heard as a child but we don’t hear these days – everyone has to carry their own cross but God (we were told) doesn’t ask us to bear more than we are capable of. In response much more recently, a Xtian pastor exposed to the horrors of SSRIs remarked that Xt never had to endure the horrors SSRIs can visit on folk.
You, occasionally helped by doctors, have been the people doing the Science that SSRIs and other drugs open the door to. You are increasingly likely to be left on your own to do real Science – See The Miracle of Artificial Intelligence.
tim says
This post is so important.
As soon as I heard these proposals, the thought that important changes in litigation are to be introduced, apparently without consideration of the fact that more drivers are likely taking SSRIs/SNRIs/ADs than any other class of prescribed drugs.
To avoid miscarriage of justice it would seem self evident that those drafting and amending the revised Driving Laws are fully informed that these drugs induce alcohol intake excess which would not otherwise occur.
The disinhibition, emotional blunting, and suicidal ideation induced by ADs might also be a contributory factor in the causation of RTAs (Road Traffic Accidents). Inevitably and tragically, this could include fatal outcomes,
Thirdly, (as stated above) The wide range of visual disturbances caused by ADs may not be detected on routine optical assessment, nor identified during the more detailed DVLA specialist eye testing.
Do these specialist DVLA Optical Assessments always record all prescription medication taken?
As an elder driver, a doctor, and a family member of a household in which all day to day activity is dominated by the results of medical ignorance of AKATHISIA, its sequelae and misdiagnosis, I have no misgivings about regular eye tests for the public and my own/my family’s safety.
I am profoundly concerned that the prosed ‘safety’ legislation appears predestined to omit the potential importance of ADs in RTAs.
It seems that vital information re AD adverse reactions remains (if not denied) poorly understood by prescribers, patients, families, the Legislature and police???
Shame on the KOLs who have promoted these drugs and downplayed the adverse outcomes.
How can an inquest produce an accurate verdict about a fatal RTA without identifying whether or not the parties involved were taking prescribed medication which may have been wholly, or partially causative?
annie says
‘Everything we know about the treatment related effects in this post has come from people like Anne-Marie, Leonard and other Lonesome Heroes – left abandoned by those who give the orders to struggle beneath an extraordinary load.’
Funny how the mind works and things come back in to your memory which have lain dormant for such a long, long time.
I am in my early seventies now, and I hope I do all the right things. I have an annual sight test which I tell the DVLA when I receive their three year form to keep my driving licence. If there is any fault with elderly drivers, it is not their fault, it is that elderly drivers don’t get a follow-up from DVLA as to why they have put on their form they don’t get regular eye tests. Of course, most elderly drivers won’t have a clue their ‘medications’ are affecting their eyesight and eyesight loss is such a gradual thing most won’t notice until there might be a calamitous accident when someone might be killed as a result.
I have developed macular degeneration which can lead to loss of sight and is a real problem as people age. The graphs look terrible on the scans, but my optometrist informs me encouragingly that for my age my eyesight is remarkably good and I pass, on her tests, with flying colours to drive.
However, night driving is impossible, as the very bright headlights come at me, leave me blind for several seconds and at that point I could crash.
With all the medications people are now on, eyesight must be one of the leading side-effects of the drugs people are now on.
Seroxat was one of those drugs ‘ left abandoned by those who give the orders to struggle beneath an extraordinary load.’
If you gave Seroxat, then may Leonard Cohen, fall on top of you.
“Ring the bells that still can ring.
Forget your perfect offering.
There’s a crack, a crack in everything
That’s how the light gets in.”
My bit of stuff about Seroxat and alcohol came to pass when I got to 4.30pm when I allowed myself a glass of wine. The cravings for alcohol grew and grew and how I got to 4.30pm I still don’t know. Never before had I craved anything. I had no idea of what craving was until Seroxat.
So at 4.30pm, we sat in the garden, and our new black labrador puppy leapt up at me and his tooth scored a long rip in my little finger. I phoned the surgery and the practice nurse said, Annie you have been drinking.
It could be said that a lot of nicely refined people might take a glass or two at the ‘cocktail hour’. I was found out by the practice nurse who, from then on, with the lady doctor, were so belligerently hostile about Seroxat and cold-turkey that all hell let loose.
This post will elevate Lonesome Heroes can work Miracles to new heights of awareness and bring it all on because it is too awful not to do so.
Idi says
There is no crack where the light is not getting in. What am I to do? Is there a light? Or only echoes of Morrisey?
annie says
Keep an eye on the cracks..
Amid cries for retraction, a medical journal reviews a discredited, 24-year-old paper on an antidepressant
The Journal of the American Academy of Child & Adolescent Psychiatry is reviewing a study of Paxil
https://www.statnews.com/pharmalot/2025/08/25/antidepressant-paxil-gsk-medical-journal-children-adolescents-depression-ghostwriting-retraction/
Amid demands for retraction, a leading medical journal is reviewing a study published in 2001 that touted the benefits of a depression pill for adolescents, but was subsequently discredited and became the focal point of a searing controversy over inappropriate marketing of the medicine.
The study, which was published in the Journal of the American Academy of Child & Adolescent Psychiatry, made upbeat claims that Paxil was safe and effective for young people. But the underlying data were later found to be misleading because they distorted results, and the study downplayed information that some patients experienced serious side effects, such as suicidal thoughts.
Meanwhile, GSK, which sold the pill, had attempted to use the findings as a marketing tool to persuade doctors to write more prescriptions, even though Paxil was not approved to treat teens at the time. In fact, the Food and Drug Administration never approved Paxil for this population and issued a warning about suicidal thoughts for this type of antidepressant, known as a selective serotonin reuptake inhibitor, or SSRI.
The Light came to the Adults..
annie says
Wendy Burn CBE (She/her)@wendyburn·
Aug 31
Strange how we have a lot of people on SSRIs in the UK and very few mass shootings…
Aug 28
RFK Jr on the mass shooting in Minnesota: “We’re launching studies on the potential contribution of some of the SSRI drugs and some of the other psychiatric drugs that might be contributing to violence.”
There is a lot of anti, in the media in the US and beyond, about these new studies.
Johanna says
On the subject of balance (and vision): The latest issue of JAMA Health Forum features a rather alarming article by Thomas Farley, MD on “Risky Prescribing and the Epidemic of Deaths from Falls” in U.S. seniors:
https://jamanetwork.com/journals/jama-health-forum/fullarticle/2837039
It reports that “in 2023, more than 41 000 individuals older than 65 years died from falls … More importantly, the mortality rate for falls among older adults in the US has more than tripled during the past 30 years. In contrast, death rates due to falls decreased during the past 30 years in other high-income countries.”
The only risk factor for falls that has clearly skyrocketed, Farley says, is prescription drug use. Especially four classes of central nervous system drugs: opioids, benzodiazepines, gabapentinoids and antidepressants. While there’s been at least some decline in benzo and opioid prescribing, that’s not true of those other two categories:
“Between 2006 and 2018, prescriptions for gabapentin and for combinations of gabapentin and opioids increased approximately 4-fold.8 And between 1999 and just before the COVID-19 pandemic, the percentage of older adults (>65 years of age) taking antidepressants increased from 8% to 20%.3 … Some older adults have severe depression and benefit from antidepressants, but it is hard to imagine that is true for 1 in 5.”
annie says
My dear mother was put on an antidepressant when she was 89 years old. She had a fall in her sitting room and was ambulanced to hospital. By the time I got to the hospital from Scotland she was obviously to me going through a bad withdrawal. She was having vivid nightmares whilst awake of drowning, suffocating and was completely distressed. For a few days I did everything I could to bring her back down to earth, reassuring her, holding her, talking to her. I didn’t even bother telling anyone about Citalopram withdrawal, nurses were scarce, they were too busy putting trays of food on bed tables where there was no chance that it would even be touched. The ward was full of the old, lying comatose or muttering to themselves.
Two weeks of this and mum slowly recovered. She never went home again. The doctor had seemingly prescribed an antidepressant because she was lonely. Mum had called me and said she was so sorry she was given antidepressants by her doctor especially after she had spent months staying with me over the two years during my Seroxat cold-turkey epic nightmare.
The nursing home worked very well. The antidepressant prescription had totally disappeared, nobody but me knew of her abrupt cessation and resulting cold-turkey.
The nursing home was gorgeous, a rural old farmhouse, with new annex, in the country and soon after she entered they threw a lovely celebration of her 90th birthday. She seemed content and happy and I spent a lot of time with her down in Kent.
Coming up to 95 years old, she was on no medication for anything as there was nothing wrong with her. I’m not sure what happened but on my next visit she was on Gabapentin, Fentanyl patches and Morphine and the doctor said, ‘it is what it is’. He also said, we considered giving her an antidepressant but we thought if we did we wouldn’t know what is wrong with her.
My mum suddenly died when I was giving her soup.
We had often talked of her 100th birthday and she had been looking to it but 95 was her lot. The senior nurse who had given her the morphine just before she abruptly died, suggested I might go to the local surgery and ‘get something’ for my grief.
I walked away from the nursing home thinking the world has gone utterly mad, me from the Seroxat, and mum, who was equally let down. What did they all think they were playing at?
Peter Selley says
Leonard Cohen himself had a history of antidepressant use and died from a fall aged 82 in 2016.
In a study of different antidepressants in the elderly in 2011, citalopram was shown to be associated with the highest adjusted hazard ratio (1.7) for falls, but risks were similar for all of the SSRIs.
Perversely, older people with falls are more likely to be prescribed antidepressants.
Lose, Lose.
https://www.bmj.com/content/343/bmj.d4551
https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-020-01730-5
Dr. David Healy says
I wonder can anyone find out what Leonard had and when and what he made of anything he had?
The falls and the elderly is interesting. Psychiatric Drugs Explained (PDE) says that older tricyclic antidepressants can cause falls because they drop your blood pressure. This was and likely still is the received wisdom but take them off their tricyclic and put them on an SSRI – which doesn’t drop blood pressure – and it now looks like you make things worse.
The only bit of a redeeming feature in PDE is that it mentions lithium cauaes falls with no mention of blood pressure – in a dramatic account the woman who brought this to my attention mentioned that the first time she knew there might be a risk was when she fell down the stairs.
D
Harriet Vogt says
A lovely piece (part of) on/by the ‘Godfather of Gloom’ :
‘Leonard Cohen is the high priest of pathos. His voice exudes misery. A suicidal Kurt Cobain, when describing the most melancholic place imaginable, in his dirge ‘Penny Royal Tea’, sang of a ‘Leonard Cohen afterworld’ where he could ‘sigh eternally’. Cohen is used to this reputation. Even the 67-year-old singer says his record company should give razor blades away with his records.
But two years ago, for no apparent reason, the veil of depression lifted. For the first time in his life, Cohen sighed, looked out on the world and felt at peace with it.
‘There was just a certain sweetness to daily life that began asserting itself. I remember sitting in the corner of my kitchen, which has a window overlooking the street. I saw the sunlight that shines on the chrome fenders of the cars, and thought, “Gee, that’s pretty.”
‘I said to myself, “Wow, this must be like everybody feels.” Life became not easier but simpler. The backdrop of self-analysis I had lived with disappeared. It’s like that joke: “When you’re hitting your head against a brick wall, it feels good when it stops”.’
It was a remarkably late epiphany. Cohen had spent the past 50 years ploughing his way through drugs, drink, countless women and several religions in an attempt to find release from this ‘backdrop’ of self-doubt. BUT THE CURE WAS MORE SIMPLE – HE LEARNED TO IGNORE HIMSELF.
‘WHEN YOU STOP THINKING ABOUT YOURSELF ALL THE TIME, A CERTAIN SENSE OF REPOSE OVERTAKES YOU. It happened to me by imperceptible degrees and I could not really believe it; I could not really claim it for some time. I thought there must be something wrong. It’s like taking a drink of cold water when you are thirsty. Every tastebud on your tongue, every molecule in your body says thank you.’
Cohen’s enlightenment did not come overnight. Since early adolescence, a sadness he can only attribute to an unexplained ‘biological reason’ has afflicted him. OVER A RECORDING CAREER SPANNING 33 YEARS, HE TRIED ALL DRUGS – EMOTIONAL, ILLEGAL AND MEDICINAL. PROZAC MADE HIM FEEL ‘SPIRITUALLY SUPERIOR’, BUT PROVED INCOMPATIBLE WITH HIS LIFESTYLE: IT KILLED HIS LIBIDO. Instead, when Cohen finished touring his last album, 1992’s the Future, he decided to devote his time to his favourite drug – the Buddhist faith.’
https://www.theguardian.com/theobserver/2001/oct/14/features.magazine37
Dr. David Healy says
The problem we all have is few people are willing to say ill of the Blessed Leonard so we really don’t know what happened with Leonard and the meds. We are forced to search for the cracks through which a hint of light might get in – the impact on his libido, the alcohol use, the death by a fall.
Buddhism might have provided an endorsement of the muting effect of SSRIs – brother you are less reactive to life’s transient distraction – this is what meditation aims at. There is an element of Buddhism and meditation that is like a Sensory Deprivation tank, which is what SSRIs give to most people and some people in an excessive dose.
Without a Ouija Board to access L or correspondence where he lists things in confidence we are never likely to know leaving too many of us as lonesome heroes marching beneath an extraordinary load with little of the help Leonard – rather than Buddhism – might have been able to offer.
Everyone carrying this load has unique insights to offer that Buddhism, Xtianity, Islam and Hinduism just don’t offer or engage with. Non-engagement with this world is close to built into the DNA of most religions
D
annie says
What has always interested me most is personal growth. Starting young with none. You might become a poet, a would-be writer, a musician, a singer, a monk, a revolutionary,
I remember being in the Greek Islands on a yacht where we escaped the organised flotilla and went off on our own only to be trawled by a couple on a boat who wouldn’t leave us alone. We ended up buying them dinner in a taverna and I started asking searching questions, and Pat Reid, my current landlord, of Colditz fame, said to me, Annie don’t ask so many questions, it is not conducive to good relations.
In other words keep safe, keep your mouth shut, and bad things won’t happen.
Someone like Leonard always spoke from his heart. It often got him into trouble, he was perhaps just too honest for the world he inhabited. As a struggling poet he had all the tools to give full voice to his good times and bad times.
Being on prescription drugs was just one part of his varied chequered life. In this day and age most people will have some drugs as some part of their chequered life. Leonard threw them all away as I did when the writing was on the wall. The worrying thing is today that the young, the in-between and the elderly don’t do that and and what should be a part of a journey becomes a lifetime’s journey.
Starting off as a poet gives you a certain edge of expression that is lost on most people and being at the beck and call of ssris and the resulting loss of realism comes to some of us and not to others. Leonard has a morass of critics, and most may be aware of his shortcomings none more than himself.
He aspired to personal growth and that is why I found him when I was young. In our student houses he was on non-stop with the likes of Neil Young and Bob Dylan. That is how we grew up.
Dr. David Healy says
Annie
We don’t know he didn’t restart them. He was drinking while meditating and had a lethal fall
D
Harriet Vogt says
I’m very willing to say ill of the Blessed Leonard – I think, and always thought, his music is literally the bitter end. But his lyrics are interesting as poetry – and he was kind of charismatic as a man.
I bet you’re right re the emotional distancing – non-attachment – that is fundamental to Buddhism. Sort of spiritual SSRIs.
But, my sense is that – ofc there are many tangible reasons why human beings feel miserable. But compulsive self-analysis is a sure way to feel even more so.. Being has to some extent to be instinctive – otherwise it’s like over-focusing on walking down stairs – you fall.
Nowhere is this more obvious than cruising around tiktok, listening to young folk in particular , fixating on their diagnoses and manifestations thereof. If we banned the words ‘mental health’ I expect we could stem something of the tsunami.
LC was apparently not taking antidepressants when he died – but who knows whether past use had done for his vestibular system. He did have leukaemia and back problems – so I guess ,in the end, he was frail and mortal.
Anonymous says
It is interesting to learn that Leonard Cohen had a history of antidepressant use. (But perhaps not surprising, if you’re a fan of his music.) He also had a storied history of alcohol misuse, including introducing it into his zen practice when he engaged with Buddhism in his late sixties. He and his master, Roshi, would ritually drink whisky.
This is a really important piece: for the elderly and others with compromised eyesight, and also for those susceptible to alcohol misuse. SSRIs have clearly had devastating consequences for Leonard, and it is a tragedy that UK legislators continue to ignore the growing body of evidence concerning the alarming side-effects of SSRI medication.
annie says
Some bits of the truly great Leonard
What Leonard Cohen Can Teach Us About Depression
Chris Aiken, MD
A recent study shows that meditative practice is surprisingly effective for bipolar depression. The late poet helps explain why.
https://www.psychiatrictimes.com/view/what-leonard-cohen-can-teach-us-about-depression
Leonard Cohen had a problem, and the medications weren’t solving it. “I’ve taken a lot of Prozac, Paxil, Wellbutrin, Effexor, Ritalin, Focalin. I’ve also studied deeply in the philosophies of the religions, but cheerfulness kept breaking through.”
The “cheerfulness” Cohen complained of was a wry euphemism for something darker. The poet, novelist, and songwriter had “dealt with depression ever since my adolescence. . . Moving into some periods, which were debilitating, when I found it hard to get off the couch, to periods when I was fully operative, but the background noise of anguish still prevailed.”
By his mid-60s Cohen had been through several hospitalizations and tried tricyclics, MAOIs, second generation antidepressants, and anticonvulsants without success. Despite releasing one of the most successful albums of his career, The Future, he found himself “really, really low, on many medications . . . I pulled my car over to the side of the road. I took out all the medication and threw it out the window.”
Leonard Cohen. Oh, boy, what a guy. Dance Me to the end of Love, was so brilliant, as was the video.
https://www.youtube.com/watch?v=NGorjBVag0I&t=1s
I have watched documentaries on Leonard, that super-sexy guy with the eyes of a defibrillator, who could charm the pants off those who find him morose. A film about his life in Greece, was spellbinding.
A bit more of Leonard
https://www.youtube.com/watch?v=FAoHYBpj8vY&t=377s