Better Times Will Return © Josie Russell 2017
This post is by our warzone correspondent Harriet Vogt from frontline trenches.
A few weeks ago I was invited to join an online discussion with a group of experts on iatrogenesis who have an in-depth knowledge of antidepressant withdrawal and the risks of polypharmacy.
These highly informed, articulate, empathic medical experts were people who come together regularly to validate each other’s experiences of withdrawal, to share insights about tapering, to offer a virtual embrace to those who are in a phase of extreme suffering. Eight members of this group have between them accumulated 82 years of inescapable post acute withdrawal – with attendant job losses, relationship ruptures – and existential fear.
They are members of an antidepressant withdrawal support group set up by Shane Cooke, and his ex-foster mother, Mary Hennessey. Shane’s own life was all but destroyed by an extreme and medically misdiagnosed and mistreated reaction to paroxetine. His story is told by Mary, including Shane’s stated purpose for their group. See Gripped and Discarded by GlaxoSmithKline.
‘He (Shane) still has a wish to “give back for all the help I’ve had” and to this end, with my support, he set up a peer support group for anyone withdrawing from antidepressants’ .
Shane, in my few brief encounters with him, radiates ‘goodness’ – not the bitterness and, quite frankly, rage I would feel in his position.
Shane and Mary originally conceived of their group as a collaborative endeavour with doctors and patients. DD and AA groups, similarities and differences. But they have had to do a volte-face. As Mary explains:
‘The greatest shock for us has been the number of people who are going through withdrawal unsupported and keeping well away from their doctors due to the medical lack of belief in the suffering endured and, seemingly, a lack of confidence in supporting them in their withdrawal… The ideal of collaborating (patients and their doctors) has had to be abandoned – in favour of BEING THERE FOR THOSE WHO SUFFER ALONE’.
Those Who Suffer Alone
Let me touch on a few of the stories of those whom I met.
T – glimpsed through a veil of tremor. Permanently afflicted by iatrogenic Parkinsonism, possible cause – valproate. But she is prescribed 5 drugs in total, so who knows? Seemingly not her psychiatrist, who recommended taking her off all 5 rapidly over 6 months, a recommendation she resisted. There is no mention of tremor in the Epilim PIL.
Yet, for anyone who cares to look on RxISK’s Drug Search Tool, Tremor has been reported over 3000 times in association with valproate. The FDA database on which this tool is based estimates that perhaps as few as 1 in 100 of the problems that happen get reported – which means we might have 300,000 cases in the US alone. It makes sense to stop valproate and see what happens – see Juggling our Bodies and Our Selves.
S came off sertraline cold turkey and was catapulted into a medical catastrophe of whole body tremors. Her GP seemed unable to grasp an iatrogenic trigger and packed her off to an equally flummoxed psychiatry, only to receive the inevitable unhelpful diagnosis of FND.
Yet, for anyone who cares to look – ‘shaking’ is mentioned in the PIL as a withdrawal symptom, along with tremors and seizures in a widely read Medical News Today piece as a feature of sertraline withdrawal.
K was prescribed mirtazapine and suffered life constricting vestibular adverse effects – dizziness and vertigo that left him unable to function. He lost his job and remains unable to work 6 years on. Can’t be the medication, said his GP.
Yet, for anyone who cares to look – in this large-scale Review of Ototoxic Drugs, mirtazapine features as a drug that commonly causes vertigo and dizziness.
The group embodies so many individual stories of harm – I can’t do them justice.
S benefitted from venlafaxine after the tragic death of her son 20 years ago, but is now only able to tolerate a dose reduction of one tiny bead at a time, if she’s lucky.
On the surface, M is sharp, immaculately turned out and professional. In reality, after enduring a decade of medical mismanagement, she has been forced to take control of her own taper – and hide her suffering.
A beautiful young woman, K, has been driven to secure an official, assisted dying agreement after multiple experiences of akathisic hell. The only way she can face living in the shadow of akathisia, is with the option of dying.
J was clearly in the throes of akathisia during the group, having been both, her word, ‘poly drugged’ and advised to do rapid tapers. Her condition felt precarious.
Anyone who frequents this RxISK space will understand what has happened in the antidepressant ‘market’ – because, to the detriment of many patients, we are looking at an endeavour that is primarily commercially driven. Vested interests, the uncritical intellectual conservatism of many in the medical profession, the collusion of politicians – have converged to RUPTURE fundamentally the essential patient-doctor relationship at the heart of good medicine
See Challenging My Doctor to Disclose. When doctors are more likely to believe a marketing script embedded in ‘the guidance’, than the tangible suffering of and often better medically informed human being in front of them, we are all at risk.
Repairing the Rupture
When the Royal College of Psychiatry, finally capitulated after 30+ years, in 2019 – and admitted that not all ‘discontinuation’ from antidepressants was ‘mild and short-lived’, but could be withdrawal, I was naïve enough to believe that this was THE BREAKTHROUGH. That patients would no longer have to suffer alone.
But a recent piece of research exposed the reality:
‘Over the last 5 years the number of people who have given up on their doctors and turned to Facebook sites to get advice on how to come off antidepressants has grown from 110,000 to 190,000. 1 in 6 are NHS patients. The growth is about 10% per year. Neither the psychiatry nor the GP College has yet provided formal education for its members on how to safely stop drugs.’
Instead of a logical move towards developing withdrawal support services – and despite the superhuman efforts of some individuals – the system seems to have stalled. Even slipped backwards, with lots of semantic and statistical lap dancing denial from invested psychiatrists – as seems to be the way with paradigms that are resistant to shifting, especially if there’s nowhere to shift. No new, easily commercially scalable (psychedelics clearly not) drugs to replace SSRIs.
THE RUPTURE is insidious – especially in psychotropic medicine – where attention and sensitivity to our expressed state of mind is key because it is THE EVIDENCE. We’ve seen how many, including members of Shane and Mary’s group, have retreated from the risk of interaction with an ill informed medical profession to suffer alone. One harmed person, TG, described this as being left in ‘a void’. Another the ‘existential shock’ of being effectively poisoned and discarded, as a sort of inconvenience. And this is a fundamental point. Once we are reduced to a state of long-term SSRI induced ‘dysregulation’, most prescribers have no idea how to help us. There’s no guidance on that.
The worst and all too familiar outcome – and one that over 75% of us in withdrawal Cosci, Chouinard and Chouinard found in a recent study – is the misdiagnosis of withdrawal or other adverse effects as ‘madness’. Even if we have the strength to hold onto the person we know we are, we can be left doubting our own sanity.
This is the most venal manifestation of THE RUPTURE, the risk of a human being disconnecting from our sense of self. Listen to LG, a survivor from Shane and Mary’s group:
‘I am tapering venlafaxine VERY slowly (currently by 3% every 4-6 weeks) and the withdrawal symptoms are severe and extremely distressing. But I don’t dare admit this to my GP. They won’t support me with any action not sanctioned by the local psychiatry team who have said under NO circumstances should anyone break open venlafaxine capsules to reduce the dose more gradually. Due to years of being misdiagnosed and gaslit by the psychiatry team I cannot bear to engage with them anymore. I have lost all faith in their medical knowledge. They don’t have the communication skills or empathy to listen to me as an expert in my own health. So I struggle on alone and unsupported by the medical profession that has harmed me beyond description.
I’m so grateful for Mary’s group, which is a beacon of light – a gathering of caring souls who have all been abused and traumatised by the awful psychiatric system which is in an utter mess, filled with “professionals” who haven’t a clue what they are doing and are entirely oblivious to the huge harms to patients they are doing with grossly inappropriate prescribing and non-existent deprescribing knowledge. It’s devastating.’
Listen to TG again:
‘Interactions with Doctors started to get twisted, I still needed help but I couldn’t trust them. I had a monumental seizure from a fast taper and it took 6 years for it to be investigated properly. I had mental illness diagnoses on my file that prevented the Dr from listening to what I was telling him about the seizure. Instead of asking me about it, he asked my boyfriend if he had witnessed it. I was being accused of making it up. He wanted to go further in disrespecting me, he wanted to push a psych assessment after i explained my chronic hypersensitivities due to the taper.
I started to feel mad. I had withdrawn from many things and I knew what a withdrawal felt like. But chronic self doubt and lack of trust in my own instincts started to kick in. In that time I developed all sorts of weird symptoms, which I’ve heard many others in withdrawal describe, many of them people who work in the field of psychiatry themselves. It was only when I started to hear it was happening to them too, years later that I started to be able to reason with myself that I wasn’t mad.’
I struggle to understand how the best intentioned, GOOD DOCTORS, can be so alienated from us, their patients. GPs seeing an average of 37 patients a day contextualises it a bit. Commercially driven ignorance and vested interests explains it more. A huge helping of cognitive dissonance is certainly involved. Those who believe themselves to be healers dispensing life saving medicaments to the sick – which most are – cannot square in their minds the fact that they can also be causing sickness and dispensing poisons.
‘It’s a bit like someone being given the Eucharist having an anaphylactic reaction to the gluten and dying .Who is going to believe God could have killed someone? ‘
We all recognise the systemic problems – although there is no substitute for being present with harmed patients to sense and feel the depth and dimension of suffering. Words are inadequate, the playthings of patient information leaflets.
Peer support groups like Shane and Mary’s are sanctuaries for those on the run from professional help. But ironically, this means those of us suffering the most are off the medical radar and the system is not forced to face up to the scale of harm. That is why, for all those who feel strong enough, and only then, it is important to be counted.
It is important to add your real diagnostic codes to your medical records – Snomed Your Doctor.
One observation from Shane and Mary’s group gave reason for hope. A small number had found unexpected support from a healthcare professional. K from a knowledgeable pharmacist (pharmacists in my experience are often a good bet – their professionalism is self-evidently tied to knowledge about drugs, rather than their egos to treatment success). C, having despaired of her usual GP, had connected with a senior partner in the practice, who declared herself ‘open-minded’, ‘knowing nothing’ about withdrawal – a state of honest ignorance C is working hard to correct.
These seemingly rare healthcare professionals need public recognition. Add their names to the a RxISK Map – a relationship based medicine map in this case locating withdrawal aware practitioners.
It is encouraging to see one humanitarian politician, Lord David Alton, leading the charge for antidepressant risk awareness in Parliament. Less encouraging seeing others’ inaction. If, for one moment, we can lay aside the terrible human cost of antidepressant harms in our society, then the disability costs may of interest to politicians:
‘I cannot speak for the others but I have lost two jobs, government pensions, future earnings and career progression with little hope I will return to the workplace again. I am 58 and still suffering daily struggles with physical damage.
Although my marriage survives it is only through previous financial planning that I have not lost my house. My wife is disabled and she now supports me having previously lived with the security of my financial potential.
The consequences reach far and wide and I might add that I have been a burden on the care system for the last 7 to 8 years with endless tests, doctors appointments, private consultations and investigations into a wide range of symptoms that I continue to manage daily.
I also was admitted to a psychiatric ward for 2 weeks in severe withdrawal and then remained under the care of a team of psychiatrists for 2 years afterwards.
All of this multiplied by many thousands if not millions of similar cases contributes to the burden of the care system today.’
Rather like a prayer, let us end on a quote from Mary:
‘Being face to face on Zoom has given people the POWER to semi-publicly CONFRONT their needs, our hope is to get them out of the darkness into the light of their RIGHT to be heard, without prejudice – even by their doctors!’
Coda
There is no clearer demonstration of the root cause of the RUPTURE than an Eli Lilly study designed to guide its sales reps on the characteristics of the doctors they are selling Zyprexa to.
All marketing uses segmentation. Car salesmen know they have two big segments – women ask about the engine while men are concerned about the color.
Doctors can be segmented into 4 groups along 2 underlying psychographic dimensions:
- The extent to which they are experimental early adopters and high dose prescribers of new drugs vs more cautious, rule bound followers. This is based on ‘Diffusion of Innovations’ theory.
- How they use information to drive their prescribing decisions. This tells companies how to optimally ‘package’ sales rationales.
This gave Lilly 4 groups to target with different messages about Zyprexa
- High Flyers: Go for it Doc, You’re the expert
- Skeptics: Docs who want to see the evidence
- Rule-Bound: Docs who follow Guidelines (so we get Zyprexa into Guidelines)
- Easy-Lifers: Docs who want things simple (so we make a once daily dose that melts in the mouth – Zyprexa wafers).
This standard marketing practice rings alarm bells when we learn that the ‘High Flyer’ is the primary target in terms of susceptibility to company messages and volume sales, and the others will follow his example.
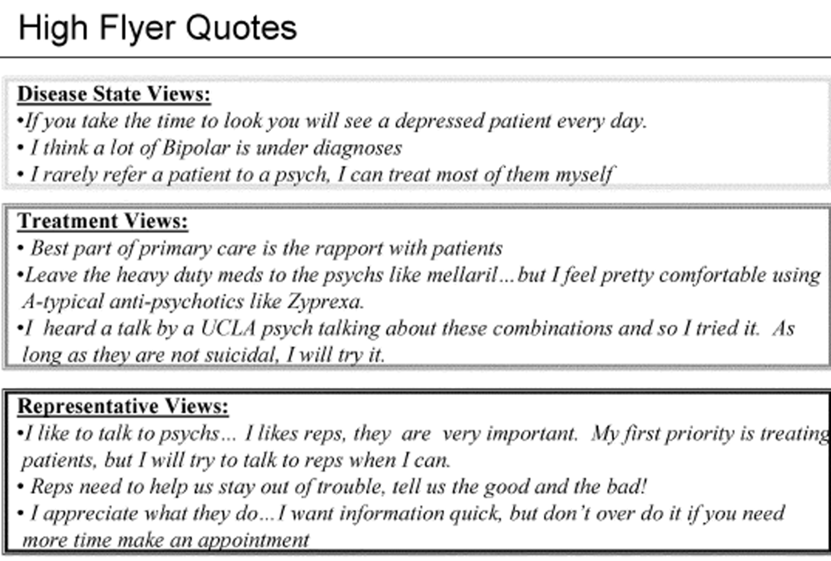
Is this a doctor who listens attentively and works in an equal partnership with their patients? No. It’s a risk taking medicator who will do ALMOST ANYTHING to reduce their patients’ symptoms and eagerly absorbs ‘expert’ sales patter.
Looking at the company comms designed to reach High Flyers with psychological precision – is disturbing. After years of this type of manipulation, it is no surprise so many of those in Shane and Mary’s now decade old support group are forced to ‘suffer alone’.
The points outlined here are colored by Zyprexa but companies take a similar approach to all doctors for all meds suitably adjusted for the condition in question. It’s worth researching this – others have segmented doctors into animal types where High Flyers become Wolves.
Tell us what your doctor is like and think about segments that might apply to the doctors you have known.
chris says
A relative new to all this asked me what FND is, hope am correct here:
diagnosis of FND = Functional Neurological Disorder
The only help I had from a doctor to come off the drugs was to make sure there was a grove in the pill so I could cut them in half and help sever myself from them
https://m.youtube.com/watch?v=HLwAYNszXpI
For me it’s beyond repair we need to be cut loose, psychiatry needs to be abolished, pharma brought under control and corrupt politicians exposed.
Dr. David Healy says
Chris
FND today means Hysteria.
You rreactions are all too understandable but risk being counter-productive. In 1962 it seemed sensible to get industry to prove their drugs worked but this has led to the invalidation of your point of view that is at the heart of the problem outlined here.
It made sense to have drugs available on prescription-only and suggesting they might be available over-the-counter sounds crazy – but we manage many dangerous drugs like aspirin and ibuprofen pretty well over the counter and having other drugs on prescription acts to make them seem safe when they are not.
Psychiatry is busy abolishing itself, so you can leave it to one side. What about abolishing FDA and MHRA – they seem to be doing more to endanger us than keep us safe at the moment?
But the real point behind the post is not who to abolish – but why do so many normal people act so disempowered – why do they fail to stand up to doctors. What’s wrong with Us?
D
chris says
In a psych hospital if you stand up to them you run the risk of being forced drugged by injection so people lie and tell them what the want to hear and do their best to get the hell away from it all. The general public have no idea how much power psychiatrists have over the public when they become a ‘patient’. And even if you do try to stand up and make a serious complaint as I did you find it’s all rigged against you.
What about abolishing FDA and MHRA – they seem to be doing more to endanger us than keep us safe at the moment?
Yes abolish them as well no question.
Dr. David Healy says
Chris
You are absolutely right that none of the public appreciate the power shrinks have. Shrinks don’t realise it either. The police when they coma on a psych ward and see what happens say we would never be able to do this.
Still the point behind this post is mostly to do with family doctors – who also wield power. If you don’t take the statin I think you should have I will throw you off my list.
Why in God’s name do we put up with this?
D
Shane Cooke says
Thank you Harriet for writing this article and joining us at one of our meetings. It’s a really good article and I hope it gets shared across the planet for all to read .
Harriet Vogt says
That’s great to hear, Shane, thank you. One of the main purposes of the piece was to honour you and Mary, the work you’ve been doing for the last decade to support patients in withdrawal – as well as to honour the individual members of your group.
What your experiences should be saying to the outside world is – if you think that because some doctors can now intone the words ‘antidepressant withdrawal’ and ‘deprescribing’, patients are in safe hands – YOU’D BE WRONG.
As you know yourself, the issue that David raises is the big one. How can individual patients – who are categorically the experts in how drugs make them feel, particularly psychotropics – insist doctors pay attention to them- and not the marketing embedded in the guidance and subsequently in their probably rather self-satisfied student minds in med school?
It’s hard for patients to stand up to an historically paternalistic and authoritarian profession. As Lucy and Chris are both saying, there is a fundamental power imbalance, especially in psychiatry. Who would blame iatrogenically harmed patients – the poisoned – from never wanting to go near their doctors – the poisoners – ever again? Not me, that’s for sure.
And yet, once again, it falls to patients – and the few like David who have our backs – to go out there and force change. Just as it has fallen to the benzo harmed, the thalidomide harmed, the valproate harmed, the vaginal mesh harmed etc. etc. etc. – to make the system listen to us.- and not itself.
Grand motivational statements are all very well – but how do we actually do it? Not easy.
I guess there are two ways. What might be called ‘instrumental’ ways – like infiltrating the bureaucratic aspects of the system, by speaking in its language. For example, by making sure that we have official medical codes for drug harms and insisting that these are added to our medical records and counted. That way the system can recognise that antidepressant withdrawal or PSSD is a significant and pervasive public health issue.
That, as we know. is the point of the Rxisk Proforma. Let’s use it – what’s the worst that can happen?. The point is – we can put anything on our records. They are OUR RECORDS.
The other ways might be called more ‘emotive’ – using our instincts to decide if we feel psychologically comfortable with our GP – and if not, changing them. Of course, psychiatric inpatients are not afforded this human right, as far as I know. But they should be – more than most.
The bottom line for me is one of attitude. I work with and have great respect and even affection for some members of the medical profession. However, when it comes to treating me or someone I love, I perceive them with a particular mindset. I am the customer and they are serving me. I have paid for their services through my taxes – and I expect to be heard, treated as an equal, consulted respectfully about any interventions. They are effectively health consultants, in the business sense, and I know what I find acceptable.
Of course it does mean that some doctors are bemused, others alienated., some repelled. But the doctor who will be the one for me and you, is the one who responds well to this kind of democratic, 21st century, demanding , customer-patient oriented approach.
Patients – and of course it’s very very hard when they/we are harmed and fragile – need to take back our power. Our minds. Our bodies. Our lives.
Lucy Green says
David, you make a very good point – why do we put up with all this from doctors?? Because, of course, there is a monumental imbalance of power. As a nurse myself for many years, I have struggled consistently with the power imbalance at work – most doctors are supremely assertive and overly sure of themselves, and this is bolstered by their medical training and senior colleagues. For psychiatric patients, this power imbalance is magnified one thousand fold – psychiatrists are trained NOT to listen to their patients, to dismiss us as subjective, to label us with inhumane diagnoses so they can call us mad when we question their actions. I’ve had to learn how to manage my meetings with psychiatry… Don’t come across as too assertive or knowledgeable! – It will threaten the psychiatrist’s fragile ego! Don’t exhibit too much anger! – They will class you as uncooperative! Don’t express too much sadness at the agonising predicament the drugs have left you in! – You’ll be classed as depressed! Don’t sound too contented/happy! – You’ll be classed as manic! The patient’s relationship with psychiatry is like walking a tightrope over a crocodile pit; at any moment they could decide to detain you, or to stop or change the drug you are now utterly physically dependent on, whilst they deny it is addictive… The gaslighting is neverending. I pray that you are right that psychiatry is destroying itself, having destroyed the lives of countless unsuspecting human beings… Psychiatrists are monsters, the ultimate abusers, getting us to believe that their torture is in our best interests. BUT! Thanks to people like Shane, Mary and Harriet, the voices of at least a few of psychiatry’s victims WILL be heard, and there is hope… at last.
Dr. David Healy says
Lucy
I’m a psychiatrist I was never trained not to listen. What I saw happen most of my colleagues was they were told RCTs were the science of cause and effect and the view of a person the meds as to what was happening them or my view that the drug was causing what was happening to them were just anecdotal views.
We have all been turned into – as it were – women. Invisible women. Who sit around while the men do the important talking. They might say later – did you enjoy that Darling.
There is a real risk that groups like Mary’s while offering important solidarity may end up being just the women chatting and giggling in the bathroom or the kitchen. Harriet’s post hints at this.
Where does this dynamic come from? Partly because men are stronger and can punch you harder than you can punch them. But a very important part of it is mothers dote on their son’s and are the primary creators of the male ego and until mothers stop doing that things ain’t going to change. We as patients create the medical ego. They aren’t trained by someone else that way = they are trained by us.
D
Harriet Vogt says
I don’t think we patients are so much the creators of the medical ego – as the affirmers. The profession comes with built-in ego superiority. Its own hierarchical structure infuses medicine with status consciousness. Patients – we medical un-professionals – are on the bottom rung.
Doctors are ranked number 3 (behind nurses) of those most trusted to tell the truth on the IPSOS Veracity Index: https://www.ipsos.com/en-uk/ipsos-veracity-index-2022
Telling the truth is a bit rich – when many can’t seem to differentiate between withdrawal and ‘psychiatric’ symptoms. And a truly insightful patient like Lucy, who knows far more about drugs than her ‘mental health’ team, has to manage the psychiatrists supposedly treating her – and maintain a positive but bland demeanour, to avoid being diagnosed and drugged on the spot.
I know what you mean – I think – with your ‘invisible women’ analogy. And, in a sense, punching back is a way of characterising the strength we need to make doctors listen to us as equals. But, this doesn’t help patients like Lucy, at the mercy of ill informed (polite term) psychiatrists with powers of coercion and incarceration.
On a lighter note, you might enjoy this section of a letter from the CEO of the American Psychiatric Association, attempting to calm the troops after RFKJr’s anointing and the latest Executive Order:
‘Dear APA Members,
Yesterday, the Trump Administration issued an Executive Order entitled “Establishing the President’s Make America Healthy Again Commission.” Within the text of the order, the Commission is tasked with assessing, among other items, “the prevalence of and threat posed by the prescription of selective serotonin reuptake inhibitors, antipsychotics, mood stabilizers, stimulants, and weight-loss drugs,” specifically to children.
I heard concerns from scores of you overnight and today about the order, and I appreciate your feedback and engagement. Thank you for reaching out. WE KNOW FROM THE EVIDENCE AND FROM OUR OWN CLINICAL PRACTICE THAT THE PSYCHIATRIC DRUGS MENTIONED IN THE ORDER, WHEN PRESCRIBED AND USED AS DIRECTED BY PROPERLY TRAINED PSYCHIATRISTS, ARE SAFE, EFFECTIVE, AND IN SOME CASES, LIFESAVING. APA stands for evidence-based science and will protect the treatments and practices that are so vital to many children and adolescents suffering from mental and substance use disorders
With Appreciation,
MARKETA
Marketa M. WIlls, M.D., M.B.A. CEO & Medical Director
Not wishing to mock anyone’s given Christian name – but you really couldn’t make it up.
Dr. David Healy says
Way back any little boy who was naughty heard messages like wait till your father gets home – which told him men have the power and smarts and are the arbiters of what happens. I’m pretty sure a little Irish boy will have heard this message from women like Edna O’Brien, who at the same time were standing up to a male church hierarchy.
Mothers dote on every minimally smart thing a son might say – more than on anything their daughter says. They elevate him and make her invisible.
It was likely confusing to a lot of boys, even back then, who on another level figured girls were smarter and more observant than them. Exam results and university achievement have since shown this to be true.
Now we have ever more professional women and ever more women than men on antidepressants and stuck in Lucy’s position. Why?
This doesn’t just drop out of the sky. Women take themselves to doctors more than men and accept their solutions.
Men don’t go – partly because they figure if they show weakness the women in their lives will use it against them. Men are now getting sucked in by maneuvers like blood tests showing raised cholesterol and being told you will be struck off my list if you don’t take a statin – ditto vaccines – and the problems these cause trap men in the system.
It’s unfair to bring Mark H into the frame, but when dealing with the problems that result from meds, women have made Mark into an epic figure. On most indices it should be Anne-Marie Kelly or Katinka Newman, not Mark, who is the epic figure. Anne-Marie got off meds as difficult as Mark’s in the face of greater opposition than he faced and she nailed down solid scientific findings unlike the hyperbolic stuff – but women do not celebrate her or Katinka. Why not?
Just as they create the patriarchy, women are now creating an Iatriarchy. They credit Mark’s credentials rather than Anne-Marie’s example. They credit the very thing that then ignores them.
I used to be an interviewer for medical posts. When political correctness required us to ask every candidate the same question, I hit on – Tell me about a mistake you’ve made. The women immediately offered any number of mistakes – the men looked blank, maybe mumbling yes I’ve made one or two but I can’t think of any just now.
Its not medical systems that trained men this way – it’s their mothers. Eli Lilly reinforced this for both men and women, by saying having your own point of view is a mistake. Our trials show our drugs only work and cannot harm. It will kill patients if you think otherwise or indulge your patient. Women like Dr. Morgan in Tom Kingston’s case have fallen in with this.
This is not medical training. It only began a little over 30 years ago – turbocharged by BMJ. The APA statement you cite, issued by a woman, is deeply ironic. Who can possibly respect an organization whose positions are all built on a ghostwritten literature that de-professionalize doctors – who used to listen – with drugs that kill more people than they benefit?
While women often don’t seem to stand up for themselves, they do stand up for their children in a way men don’t. Again and again, I’ve had cases brought to me by mothers, who know something has gone wrong for a child (usually a son) because of a medicine and find me where their lawyers haven’t. These tiger mothers are invariably right.
This is the real meaning of Care – its not wiping bottoms its standing up for someone when it can be scary to do so. At this point we need to ask Why Can’t Men be more like Women? Why can’t Women be more like Women when it comes to themselves? Why can’t they celebrate Anne-Marie or Katinka Newman? Why didn’t Dr Morgan attend the inquest and tell the coroner – you know the only way to explain Tom Kingston’s death is the meds I put him on killed him? Caring, healing, used to be the domain of women not men.
Neither of us know Lucy, so this is tricky. I have a backdoor on the fact Lucy has made some breakthroughs like Anne-Marie’s but it’s not clear she has – yet at least – chased these to their logical conclusion. Is blaming the medical system for this a cop-out?
Exactly what kind of strength does it take to stand up to APA or NICE – who concede their guidelines are based on a ghostwritten literature – baloney?
I imagine God running an interview at the pearly gates where Nicki Morgan and Richard Smith turn up – see Making Medicine Great Again – and asking Tell me about a mistake you’ve made.
D
Lucy Green says
Women are the targets of centuries of misogyny.. it takes a community to raise a child – we can’t just blame mothers for the male ego! Or patients for the arrogance of doctors! Not one psychiatrist has ever been interested in my story, let alone offered any validation or, god forbid, an APOLOGY on behalf of their profession for the mind-blowing amount of suffering I have endured – it is THEY who have sent me to HELL and back countless times, thanks to their prescribed poisons! It’s about time that men took some responsibility for their own arrogance and not try to blame women for it without trying to understand the fuller picture and the crazy pressure mothers are under to conform to the perfect “Mother Mary” stereotype! I won’t allow any psychiatrist to blame me or any other of their victims for their own failings! Doctors can have VERY slopey shoulders! They must learn to exhibit true empathy – starting by REALLY listening to theiir patients’ stories, acknowledging them, and offering a meaningful apology – in other words, showing some basic human decency! Not ecpecting patients to come up wuth the solutions to the problems THEY have created! Having said that, switched-on patients, like myself, will of course try diligently to offer insights and share experience of things that have helped us, because we can’t bear for others to suffer in the ways we have.. Have faith in us women – you might just be surprised by our determination! And never tunderestimate psychiatric survivors like me – we have FIRE in our belly, because we truly knkw how to.put LOVE into action – the greatest super power of all!! Psychiatrists beware, we see you, and, believe ne, we are not afraid of the fight.
Dr. David Healy says
The question was Where is your inner Anne Marie? Does the group you’re part of hero-worship Mark Horowitz? If so why?
Flinging the word misogyny around is cheap. Any misogyny there is likely comes from men figuring women are smarter and more verbally dexterous than the. What’s stopping you using your smarts and verbal dexterity to win out?
Was it misogyny when Nikki Morgan treated tom Kingston they way you complain you are treated?
More than half of younger doctors are now women. Are women or men putting more young women on antidepressants and psychotropic drugs? Has having more women eedics put paid to the misogyny?
What are you doing in the area you live in to go around the women medics and assuming they will agree with the misogyny idea – getting them to stand together. If as a group they chose not to prescribe psychotropic drugs to young women without access to all the data so that they can participate in a decent informed consent conversation with you and other women, the system would have to respond. Will they do it? Is it misogyny holding them back?
D
mary H. says
‘I have a backdoor on the fact Lucy has made some breakthroughs like Anne-Marie’s but it’s not clear she has – yet at least – chased these to their logical conclusion’.
You may well be surprised!
Dr. David Healy says
Great news if she has. Here’s hoping it works out
D
Harriet Vogt says
My own childhood was so intensely feminised, I understand the social reality of what you’re saying – but can’t feel it. By the time I was 8, my parents had been married to and divorced from each other – twice. There was no question of, wait till your father gets home – he was on another continent, which was fine by me. My mother and I were then taken to the bosom of her family, a wild Aussie matriarchy. Even my grandfather, a boy’s own action hero, had a tender, maternal heart.
Although obviously a generalisation, my sense is that women – heroic women in the prescribed harm space – like Katinka, Anne-Marie, Mary, Yoko, Marion, the late Christy Huff, Janice Curle and so many more – are less publicly celebrated than some blokes – because they neither need nor want to be.
As a woman – my feeling is that we tend to be more task oriented than ego driven. We want to get things done. Maybe that comes from our upbringing, our ancestry as hunters as well as berry pickers (the narrative had changed on that) – who knows? A great woman friend of mine – at various times in her life – a nurse, social worker and CAMHS therapist working with abused children, put it rather well. ‘Sh*t happens. We deal with it. Love helps’.
As you know, I’m also troubled by the huge imbalance in the extent to which women are drugged with antidepressants. There will be many layers to it – the obvious ones being our biology – periods, fecundablity, pregnancy, menopause – and emotional articulacy – the docs have more chances to capture us.
The peak age range for antidepressant prescribing to UK women, 50-59, can be a tough life stage – kids leaving home, aged parents keeling over etc. It’s confounded by indication – I gather quite a lot of AD prescribing in women of a certain age is for pain – as well as nonsensically for menopausal symptoms. And inevitably it’s upweighted to social deprivation. Drugs don’t cure poverty, but they enable doctors to see the next patient of the average 37 that day.
Like you, I simply do not understand why women accept this treatment. I think rather than hazarding a guess, that needs to be a future research project.
I suspect Mark is revered – not just because he’s an outspoken Aussie! – but because he is offering what seems to be, in theory, a fool proof solution to a life wrecking problem that he has and still experiences himself..
Commonsense suggests that a complex, dynamic biological system that has been dysregulated by drugs, is unlikely to be reset by going into reverse. Tbf ,Mark has always qualified the theory with the need to individualise. I do agree with you, though, that the existence of an apparent algorithmic solution to the management of withdrawal does allow the system to heave a disconnected sigh of relief – well, that’s done and dusted then. Even if the theory worked, the problem remains, what about the 000s of people left disabled by these drugs?
Great to hear the whisper of some progress from Lucy. All her own work I bet. Delivering a sharp uppercut to her invalidators. I was lucky to meet her at Shane and Mary’s group and look forward to an update.
I heard a smart comment from an X friend – a philosopher who was iatrogenically incapacitated – responding to Allen Frances exalting the UK’s progress on deprescribing:
‘Deprescription is harm reduction, i.e. doesn’t repair harm/sequelae already done. These guidelines should first & foremost change the adventurous practice of GPs & psychs towards prescription, not just offer a risky way-out w/o guarantee.’ @asenacide
I think we’d all agree with that.
Coda
Re – exactly what kind of strength does it take to stand up to the APA or NICE?
You know that. My grandfather did too. Never take the easy path, when it’s wrong. It helps to have moral cojones the size of planets.
Dr. David Healy says
H
It should be so easy to stand up and change the system. The entire thing is based on a ghostwritten often fraudulent literature with no-one – not regulators like FDA, EMA, or MHRA having access to the data – yet building guidelines and sanctioning drug labels that kill people = and increasingly are killing our children and disabling a younger generation especially of women.
What is hard about standing up to this, especially if we get together? What I am trying to get at is where is the outrage. Being Irish I grew up in a matriarchy. Irish women won a Nobel Peace Prize for getting together and making peace in Northern Ireland a moral imperative. No-one is going to get shot dead on the spot if they get together and protest against the Magic Bullets (medicines) being shot at us in ever increasing amounts – leading not to death on the spot to premature death. These are bullets we don’t have to be hit by – but it’s only going to happen if we organise and not just meet in a group and moan but do something rather than think someone else will do it for us.
Marks Snomed codes are an instance of this and thanks to you we now have a practical way for people to run with this – but will they? And if not, why not? Why the abject fear in the face of what is supposed to be a caring profession?
D
tim says
“It is not propaganda’s task to be intelligent, its task its to lead to success”.
“There is no need for propaganda to be rich in intellectual content”.
Joseph Goebbels. Reich Minister of Propaganda.
chris says
I agree with almost everything you say. To see the ongoing horror shows of akathisia in the media makes this all the more important to highlight and think about.
Kate says
I joined Mary’s group in late 2021 and found it invaluable to be seen and heard by those who understood and believed what I was going through.
I was in a bad way after 3 failed attempts at coming off of Citalopram and Mirtazapine.
Happy to report I’m in a completely different place today – I’m a new mum to twins, able to work, studying for a degree in Social Psychology and looking forward to my wedding in September.
I’m still withdrawing but at such a snails pace that I’m thankfully barely affected by symptoms, unless the batteries on my scales are running low and the weights get thrown off! Even though I’m down to approx 1mg of each drug, I still have 2 years to go till I’ll take the last dose, the increments are that miniscule.
I’m still in touch with Mary on a monthly basis and know that if things go awry, I can always join the group again as it really is a lifeline.
chris says
I still have 2 years to go till I’ll take the last dose, the increments are that miniscule.
Do you use the tapering strips and the hyperbolic method at the end if so how are you able to do it in the UK is it via Mark Horowitz or the chap in Holland ?
I have an elderly relative who may have to come off citalopram soon and I want to work out the best way for her and pass on the information.
Dr. David Healy says
Take care Chris. There is no one best way. What might work for you might not work for Kate or me – and vice versa. In Shane’s group people could get off several drugs without using the horowitz or tapering strips method but not get off one drug particular to them. Quetiapine was the biggest problem for more than one. At least one opted not to try any more to halt it – and a decision like this has to be respected. Someone else seemed to have been helped by antidote.
When trying to help your elderly relative with the best of intentions, beware of becoming like the doctors you give out about – someone following a guideline and not listening to the person you are trying to help
D
chris says
Yep am aware there is no one way that is best for all. I just plan on giving her information. She has tried once but failed. As far as I know she is not aware of taperstrips nor akathisia.
Kate says
I am making my own capsules by crushing and weighing the tablets.
I may move on to liquid form towards the end.
Yes, I am following a hyperbolic tapering plan.
Patrick D Hahn says
“A beautiful young woman, K, has been driven to secure an official, assisted dying agreement after multiple experiences of akathisic hell. The only way she can face living in the shadow of akathisia, is with the option of dying.”
Doctors have always had the option of burying their mistakes. But nowadays some seem in an unseemly haste to do so.
David T Healy says
To follow up on some of the points being made. Shane’s group has had the experience of someone come along who claimed to have been easily able to get off the drugs those present were having problems with – and told them it was just lack of willpower on their part. They got rid of this person as far as I remember.
This applies to Mark Horowitz also and Peter Groot. Mark had severe problems getting off and may still not be fully off. Peter Groot tried for years and failed before finally succeeding. But even Mark and Peter and notably Angie Peacock who got off can be left with enduring problems afterwards that no tapering or other method will necessarily help.
If Chris gets off a medicine I can’t get off – that doesn’t make him an expert and me not. I’m the expert on me and without solid evidence – perhaps tests for biological levels of willpower – it is all wrong for anyone to claim to know what is going on or what might suit someone else
D
Dr. David Healy says
There is an old Buddhist saying – if you meet the Buddha on the road, kill him
D
Dr. David Healy says
On the point about why someone who has had tremendous difficulties getting off and may not have fully succeeded get’s recognised asd not just the expert on him but on withdrawal generally, it’s probably worth adding that it even suits Pharma to pitch Mark as the expert.
Problem has been solved, nothing more to see here, move along. I say this having had some bruising experiences with groups like Shane’s who do not want to hear that Mark is not the expert – that no-one is. That you have to be your own expert.
D
Tricia says
I for one am very grateful to Mark H for speaking out on this issue and the work he has done.
Dr. David Healy says
No one is asking anyone not to think it’s good to have Mark. His efforts have helped raise the profile of the withdrawal issues – partly perhaps because of a mythical idea of hyperbolic tapering which is wrong but an easily digestible idea that helps persuade people there is a way forward. But holding Mark up as an icon or unique expert when he may not be fully off the meds or free of their problems himself – where others (particularly women) are is a contradiction in terms.
The problem I’m trying to raise is that it is going to take something else to really transform the state of affairs so many people are stuck in. Mark has come up with another good idea that I initially thought would go nowhere – getting people to get SNOMED codes for dependence and withdrawal included in their medical records. But many of the same people caught on meds and alienated from mainstream medicine seem too scared to do this.
This echoes the problem RXISK Reports were created to tackle. The idea was you fill a report which gives you a score indicating how likely it is your problem is linked to your med and you take it to your doctor. It should level the playing field. It shows him that there is expert evidence that what you are saying is right. And that you have recorded your problem and shown him that, so that if things do badly wrong and he has done nothing he might be more easily sued.
What happened? People filled reports in their tens of thousands but almost no-one ever took them to their doctor. It seems most people are too petrified to do so.
Ditto with a RxISK Map. We have tried to get you to report on doctors who listen and accept your view of what is happening to you so between us we can build a map that will alert others to doctors in their area who seem decent people and correct in believing you. If the ones who don’t listen. see business going elsewhere they might start listening too
But while we have put some doctors names on the map, there are far far more good doctors that none of you are reporting back on – you are not mobilizing not doing anything to help yourself. Sitting around waiting for some doctor to raise the issues in the media or with politicians is not going to do it. It needs a grassroots movement. Where is this going to come from?
D
Anne-Marie says
I totally agree we are all different. Same as I never understood measuring health from 0-10 how would you know what 10 is if you have never experienced it.
Johanna says
I strongly agree with Harriet – it makes no sense to blame women as the creators of male arrogance (and therefore medical arrogance). Throughout our lives, however, we are used to being blamed for our own misfortunes, berated and mocked as the supposed architects of our own oppression. In every case from over-medication, to lower wages, to rape. Nothing new there.
That’s why more of us are on antidepressants—not our supposed submissive good-girl nature. Too often any physical symptom (or other life problem) we complain of is dismissed as “all in our heads.” Not only does it subject us to harmful drugging – it also robs us of appropriate care for everything from heart attacks, to post-partum sepsis, to cancer.
Not to mention that us “silly obedient females” are prescribed more antidepressants for much the same reason that “ignorant hillbillies” in the coal-mining states of West Virginia and Kentucky are prescribed more OxyContin. Because we are targeted by the industry—deliberately and cold-bloodedly.
And lest we forget: Anne-Marie. Annie Bevan. Mary Hennessey. Heather Roberts, and Chrys Muirhead, may they both rest in peace. Kim Witczak. Wendy Dolin. Sally MacGregor. Katinka Blackford. Kristina Kaiser. Colleen Bell. Dee Mangin. Harriet Vogt. Nancy Olivieri. As you yourself point out, overwhelmingly the workers and the warriors around here over the years have been women.
And if some women (and men!) are overly impressed with the opinions of Mark Horowitz as opposed to those of David Healy, does it really make sense to sneer that they are just swooning over Horowitz, “because he is a man”? I mean, after all, he’s not the only man in the room …
Females, like males, have opinions. Sometimes right, sometimes wrong. Sometimes we can be sold a bill of goods. But it’s not because we have our brains between our legs, as they say, and “hero-worship” any smooth-talking man. For Christ’s sake!
A great deal of what is said here is indeed misogynist and bigoted. It is also just plain wrong and will get us nowhere. It undermines everything we have labored to accomplish for the past thirteen years. I hope it will stop. If that is “cheap” of me, so be it.
Dr. David Healy says
Jo
There are likely big differences between the US and the rest of the Anglosphere or Europe on some of these issues. The problem as I’ve tried to bring out in the commenta and posts and as you will have seen for years is that folk on these meds are not organizing themselves. A very few get together in small groups which risk aggravating the feeling of helplessness as much as offering support – risk increasing the sense of paranoia rather than encouraging people to get things done.
Mary and Shane have for a long time been trying to make things happen – get people to take action. RxISK has tried to do the same thing. We picked up Mark’s suggestion of SNOMED codes and with input from Harriet have tried to put a realistic workable process in place so people can start getting SNOMED and MedDRA and other codes into their records. But it still ain’t happening – it can almost seem like people prefer to moan rather than do something. This is not just me – a man – saying this. Many of the women trying to make things happen say the same thing.
On the other hand, set up a business and charge a fortune for life-style coaching etc and individuals flock to it and hand over lots of money -rather than get together and make something substantial happen.
Mark is great. He can be pugnacious in media interviews and he has standing being a doctor and maybe being a man. But he also symbolizes in a weird way part of the problem. The fact he says there’s an answer – which is the wrong answer for many people – means that in many of the groups there are he is idolized – he is viewed as the expert even though he hasn’t or hadn’t managed to get off stuff fully himself. This is a weird definition of expertise. Telling people that hyperbolic tapering is a great marketing idea useful for all of us for this purpose but likely irrelevant for most individuals elicits a terribly hostile reaction from most of these groups – and I’ve been liaising with far more than just Mary and Shane’s group.
The point with SNOMED and RxISK reports is to put tools in people hands – but as you will have seen, it’s dammed difficult to get anyone to pick them up and start making things happen. We need to nail down what holds people back? It seems to be partly magical thinking – someone else is going to ride in and put things right. They won’t. Things are getting worse – and they who came for our neighbours a while back are now coming for our children.
D
susanne says
Jo I agree with much of what you have said which was or could be read as insulting to women and indeed many men but would add that it is sometimes forgotten that untold numbers of people women and men are working to create a better life for all in different ways mostly behind the scenes including for the same reasons and same issues as Rxisk . These also include the un- named ‘warriors’ without whom the leaders of the gang(s) who although rightly respected would get nowhere.
It is undeniable that progress is undermined all the way but small actions are worth trying even if these are discounted as pointless or naive or because power structures make it farcical to try again . Nobody can predict if or when the knot will undo ,if circumstances or the individuals in power change…
So Call for submissions by Whitty and Co. With all the baggage he carries it is still worth chipping away
It will begin with ‘national listening events’ with doctors, trainers and patients over the next two months, which will be followed by a ‘call for evidence’ in the spring.
NHS England has announced it will conduct a ‘significant’ review of all postgraduate medical training, including GP programmes.
England’s chief medical officer Professor Sir Chris Whitty and NHSE’s national medical director Sir Stephen Powis
The national review will cover:
placement options
the ‘flexibility’ of training
‘difficulties’ with rotas, control and autonomy in training
and the ‘balance’ between developing specialist knowledge and gaining a broad range of skills.
It will begin with ‘national listening events’ with doctors, trainers and patients over the next two months, which will be followed by a ‘call for evidence’ in the spring.
This engagement process will run until June and a report on the review’s findings will be published in the summer.
NHS England said today that resident doctors, previously known as junior doctors, have ‘made it clear that they have concerns and frustrations with their training experience’.
‘As the people responsible for training doctors, there is much more the NHS and our partners can do collectively to improve their learning and working experience in the NHS.’
‘Patients are struggling to access expert medical care ………
‘There is little benefit in rearranging the deck chairs while a ship is sinking; ‘ They need help so let’s help them by submitting responses
Harriet Vogt says
I may have found a few more pieces for the jigsaw of – why women are diagnosed with ‘depression’ 2x as much as men. Apparently a common pattern found across Western and Non-Western cultures.
EXACTLY as Johanna said – and many of us sense – there is clearly an element of gender stereotyping (aka cheap ole misogyny) – where female ‘emotionality’ tends to be the go to diagnosis for actual physical symptomology:
‘Evidence suggests that emotional distress in female patients is often medicalised and that there is a tendency among health professionals to attribute physical symptoms to psychological factors more readily in female patients than in male patients, instead of looking for other attributable biological causes of their symptoms ‘
https://pmc.ncbi.nlm.nih.gov/articles/PMC10665506/#B33
The suggestion in this large study in Catalonia (supposedly 7th in the EU gender equality ranking) is that female GPs may prescribe less quickly and at a lower dose than their male counterparts, but gender stereotyping is the most significant explanation for the disparity in depression diagnoses between the sexes.
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/1733742
This isn’t surprising. But what did surprise me – although it’s obvious given a moment’s thought – is that men and women tend to express feeling depressed (let’s not reify this) differently – and the norms on which medical expectations of ‘depression’ are based are more female than male.
So, whilst irritability is supposedly a signifier of feeling depressed for both men and women – women are apparently more likely to feel hopeless, tearful, be insomniac and withdrawn, whereas the male of the species is more likely to become angry, aggressive and hit the drugs, drink etc..
This ties in with a study in Sweden which made no sense to me at first – where they found that men reported ‘depression’ more than women, but were prescribed ADs less.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5451647/
When you click on the contemporary NHS definition of ‘depression’, just looking at the psychological factors for now, they’re very female.
– continuous low mood or sadness
– feeling hopeless and helpless
– having low self-esteem
– feeling tearful
– feeling guilt-ridden
– feeling irritable and intolerant of others
– having no motivation or interest in things
– finding it difficult to make decisions
– not getting any enjoyment out of life
https://www.nhs.uk/mental-health/conditions/depression-in-adults/symptoms/
So not only do us ‘wandering wombs’ expose ourselves more to medical interventions by presenting more often (mostly driven by our biology imo), we are ,to some extent, a self-fulfilling prophecy.
Dr. David Healy says
H
I’d be wary of most of the literature in this area. Thirty years ago only a fraction of people now depressed would have been diagnosed as depressed. Depression up till the SSRIs had been melancholia or endogenous depression or featured as part of manic-depressive illness. There was also what was called neurotic depression – which was an anxiety state rather than depression.
The psychiatric system only saw the first group of disorders – the emerging psychotherapy system saw the neurotic depressions and anxiety states in general which were vastly more common than hard-core affective illness.
A century ago admissions for melancholia were slightly more common among women and for manic-depressive illness were twice as common but for both conditions were miniscule compared to now. The rates for schizophrenia were equal between the sexes then but now are 3 or 4 times more common among men – as with juvenile ADHD and autism.
The SSRIs reveal a clear interplay between many of the drugs we use and endocrine systems especially women’s. SSRIs and anticonvulsants tap into menstrual cycles and can start causing cycling. These are destructive biological effects that I find hard to see as having anything to do with emotionality.
The anxiety states though are different. Up till the SSRIs these were clearly seen as emotionality and not physical illness. If there were physical features people were more likely to be viewed as somatising. The pitch in adverts for benzos and then later SSRIs which were aimed at this market – everyday nervous problems – featured women primarily.
The argument up till 1990 was not between biology and emotionality but between psychotherapy which internalized problems into women and a more social psychiatry which saw these problems as lying more in social conditions – change the conditions women have to grapple with will do more for their mental state than anything else will the argument ran.
One problem that you may be hinting at is that women are acutely aware that social circles relax when a women says she is taking an SSRI just as they relax when a person with epilepsy says they are taking an anticonvulsant or a person with AIDS says they are taking triple therapy. Women are supposedly demonstrating control by taking their pills. In the case of antidepressants, this is very much a creation of the SSRI era.
It feels Medea or Medusa like to me – a lot of people, men clearly but also other women it seems, are afraid of the wrath of women. Clearly misogyny is real thing but is this misogyny? Or is that a loose use of the word. Are women never threatened by other women? I’ve had far more women tell me – you think we are sweetness and light but we are really malicious evil bitches (their words not mine) – adding you guys see nothing.
Being Irish offers an insight on this. England has traditionally viewed Ireland as feminine compared with rational and male England. We figure the Brits are ‘limited’ and they see us as emotional. And the first item on the agenda for Irish political movement is the split – among malicious evil political actors. There is a power element here – it’s easier for those who have the power to hang together. And pharma companies hang together rather than compete. Medicine and healthcare bickers. The golden rule is whoever has the gold rules.
This all needs separating out from Ruptures in Clinical Care. Chris mentioned how awful mental health set ups have been – but asylums began with really good intentions aimed at stopping us from chaining folk in outhouses or even killing off the mentally deficient, demented and epileptics. There was a lot emphasis on good food, fresh air and work on the farm till recovery took place.
The medical input was almost nil – the doctor in the asylum was an administrator. Where there was brutality it was more likely to come from nursing staff. But things really began to deteriorate when buildings built for 100 or 200 people ended up with over 1000 in them. When psychosurgery and ECT came along there was pressure to use them to reduce the numbers.
We are facing similar pressures now and despite the lessons of history it seems unlikely that people are going to resist the Quick Fix option. The image of depression we have now didn’t exist 30 years ago. The rhetoric that leads to treatment now – prevent suicides – applied to melancholia not current SSRI-depression. You can’t argue from previous studies on depression anymore.
None of our research applies to what has been happening in the last 5-10 years where its young women 10-30 who are most likely to be starting these drugs – nothing anybody has been thinking up till this envisaged a situation like this. That age group, male and female generally had high levels of wellbeing – notwithstanding teenage angst. Pre-SSRIs both psychotherapist and shrinks stated confidently young people cannot get depressed (get melancholia). They can be unhappy or miserable but input from an adult can sort that out. Now they are on pills. Something other than misogyny is driving changes like this.
It’s pharma marketing that has made women ‘depressed’ and the culture it has created has added young women into the mix. I’m not sure we are going to be able to stop the bodies being thrown into the river any time soon – next weeks post will speak to this. But what Mary and Shane and groups like that surely are doing is fishing bodies out. We need to build up the number of folk on the bank, female and male, who are actively fishing people out and helping them stay out rather than sitting miserably on the bank complaining about how cold the water was.
Which brings me to another woman – the heroic and extraordinary Brianne Dressen, one of the injured, who has done more than any man on the planet to raise the profile of vaccine related harms but even more so to mobilise with React19 to get the injured and their families to collaborate in putting things right on political, emotional and biological levels.
Again a woman. With folk like Brianne, Anne-Marie and Katinka leading the way, is calling on women to do for themselves what they do for their children misogyny? I can understand them being less likely to do it for their husbands.
D
Harriet Vogt says
I was using women’s – ‘emotionality’ – in an ironic way – in the sense of how we are characterised and targeted by AD marketeers – ‘stereotypically’. If stressed I get out my boxing gloves – must be channelling my inner bloke. But I understand that you’ve used it with clinical seriousness.
Taking the human condition, fragmenting it and medicalising the pieces. Can there be a more fundamental social rupture.? You rang alarm bells in ‘The Antidepressant Era’, nearly 30 years ago – and we’re still stuck in the antidepressant era..
‘While modern pharmacotherapy has offered answers to health needs on one level, however, the revolution appears to be a force for alienation at other levels’.
Likely the so caled ‘fat busters’ are ushering in the next era of alienation – from our bodies.
Of course, Johanna is right, women have always been the core target market for ADs – and, looking at it from the dark side, it’s sound commercial thinking. Even if totally healthy, our biology forces exposure to medicine more often than late presenting men, we find it easier to talk about our emotions, especially to other women. In OTC medicine, the accepted wisdom is that the woman in the household will be the key decision maker. Even Viagra comms are aimed primarily at women.
It’s all changed a bit with Gen Z` – the most medicalised and ‘mental health’ disabled generation in the history of the world. Company PR seems to have recruited ‘sensitive’ nepo-blokes, who gain kudos for being open about their ‘mental health’. And then there was that truly revolting ‘post your pill ‘ campaign https://www.instagram.com/jakegoodmanmd/p/CXHifwjPiWW/, distorting stigma to flog drugs.
Bottom line – I don’t really think male or female is a useful differentiator in drug safety campaigning. The objective, as you’ve said, is igniting the power of collective action.
chris says
“Why didn’t Dr Morgan attend the inquest and tell the coroner – you know the only way to explain Tom Kingston’s death is the meds I put him on killed him? ”
Did the coroner communicate with Dr Morgan at all?
If it were me I’d want to know what she will do when someone else comes in with a bit of anxiety and insomnia, plus if she can now recognise akathisia, is aware that there are hundreds of drugs that induce it and the ways it can be induced.
Does she now know this stuff?
chris says
BTW I’d say exactly the same if Dr Morgan were male.
chris says
“switched-on patients, like myself, will of course try diligently to offer insights and share experience of things that have helped us, because we can’t bear for others to suffer in the ways we have.”
Yeah I we want to hear it and from anyone else who has survived the horror of deluded psychiatrists and their enforcer nurses’. Just watched a 1970’s documentary “Madness and Medicine” it was appalling then, it’s worse now.
Dr. David Healy says
Chris
Here’s another angle on what you’re saying that gets away from the male-female angle I’ve imported into earlier responses. We usually see parents as educating children. But anyone who has a chance to witness what happens at close quarters, often ends up figuring good parenting stems from the child educating the parents in how to do the job properly. It should be the same with medicine – doctors should view us as the scientists turning up, each of us with different insights to bring to bear on the job they need to do, who can educate them.
The problem is they – like an increasing number of millennials do parenting – are doing it from the book rather than learning on the job and from us. On their side this is not professionalism, which should involve listening very closely to us and bringing what might be relevant in books to bear on our problem – but not forcing us to fit into the books. The problem with the bureaucratic approach shows in things like dealing with the terrible twos – where the raise your child properly gurus say it might be linked to having a second child to which the only answer is are you telling me to get rid of my second child?
On our side, we too often act like children in search of a father figure. We hand over power we shouldn’t hand over. This is part of the problem with groups like Mary and Shane’s – which play an important role by just existing but it can come with costs as many of those behind these groups know all too well. They end up saying what’s the point if people do nothing – if they just sit around and moan about the terrible parents we have.
It’s as much about growing up – changing us – as it is about changing the system. If we grow up it should be easy to say – a system build on a ghostwritten fraudulent literature where pharma play doctors, to borrow a Trump phrase, like a fiddle cannot be let survive.
Have pharma taken too much territory for us to push back? You mentioned things were bad but are worse now – they are getting steadily worse. We are not turning things around as things stand.
D
chris says
Myself and others who have been inside psychiatric hospitals and significantly abused run a real risk exposing the truth.
I’ve already flown close to the sun and been told to ‘stop complaining or you’ll be medicated’.
I sometimes wonder if one day I’ll be contacting you having been detained fearing for my life asking if you could try and get me free.
This is a very real reality. So I have this balance in my mind every time I read about the next horror show and become determined to do anything I can usually emailing about akathisia or commenting on here and else where, with the lurking fear of my past pulling the other side down.
There is absolutely no question they would drug the hell out of me.
Dr. David Healy says
That’s a real worry but not one that you alone face any more. Mandating vaccines put everyone in the firing line. That should give folk a reason to stop and think – this is not only happening to someone like Chris whom we can feel sorry for but forget, it is happening for me also.
D
mary hennessey says
Hi Chris, I think that your worry rings true for many who are going through the use of, or withdrawal from, psychotropic drugs. Our thoughts, generally, run along the lines of ‘we hear the horror stories, they happen to others – surely not to us’ BUT, if we hit the brick wall where noone seems to want to hear us, let alone help, then, quite naturally, our perspective changes. The shock of being in the grip of withdrawal means that, no longer is it a case of “it’s happening to him/her”, it becomes “it CAN happen to me”. At that point, FEAR takes a grip – and fear, of where we find ourselves, coupled with the mystery of how/ why we were let down and the roller-coaster of symptoms is CRIPPLING.
Now, to this week’s post. Harriet, we couldn’t have done this without you – your skills in getting members comfortable in your company are a joy to watch. The trust that they have in you is remarkable and I sincerely hope that we can lead them now in directions which will show our gratitude to you . It will come in seeing them start to put trust back IN THEMSELVES.
I need to add here that there is a second group, a fairly new group, called ” Prescribed Drugs Withdrawal Support Group – a peer support group”. A similar title but not in any way linked to North Wales. We work very closely as two groups. We meet fortnightly – they meet weekly. The difference, as I see it, is that we invite speakers ( inviting the other group to join us) and try to confront the issues surrounding the suffering. Some individuals use both groups – some use the new group only and some stay only with us. We could probably say that the new group is a forum whereas we are hoping for action! We are linked to the WARM Network of meetings, started by Laurie Oakley, in America, a good number of years ago. Laurie, just like us, turned to David when an expert’s advice was called for.
Before I finish, David, can I just bring you up to date that mothers no longer threaten their children with “wait ’till your father gets home”, it’s now “I’ll take your ipad off you” !
Dr. David Healy says
Mary
The iPad or its equivalent is going to feature in the next post
David
mary says
From what you say below – maybe women can read minds as well – if so, look out!
Dr. David Healy says
I know all about this super-power. But its another one I’ve been trying to bring into the frame. What Harriet calls emotionalism reframed as passionate is a superpower. It’s what mother bring into play when their children are at risk. What you brought into play when Shane was in trouble.
Harriet says doctors are made uncomfortable by it – you’d have thought women doctors should be more understanding but seemingly not. The question is how to mobilize it. It is getting harder to do so – as next weeks iPAD post will bring out – the system is becoming ever more algorithmic – with the emotional range of a stereotypical english male – varying on a 1 to 5 scale between 2.95 and 3.05
D
Harriet Vogt says
Thank you, Mary, for those kind words. It’s great collaborating with you all – and all who contribute to this space.
It would be good to get a clearer understanding of what stops us sending in a ProForma. I suspect it’s more complicated than David’s nonetheless very REASONABLE question – why are people fearful of challenging a supposedly caring profession who only fire (potentially lethal) magic bullets?
As you say, living in a state of fear is one real obstacle. Some of the people in your group are in survival mode – and there’s little room to prioritise anything else.
There are obviously other barriers. When the worst can happen as a psychiatric inpatient, you keep your head down- but we are really focussing on general practice.
I’m guessing a few, we might explore:
1. Irritating my doctor might result in them withdrawing other treatment or care I need. My health will be penalised in some way.
2. What’s the point of connecting with a doctor who caused my suffering out of ignorance in the first place – and then either denied it and/or has zero idea of how to help?
3. I am so angry and distressed by what has been done to me in the name of medical science; I can’t even contemplate being in the same room as this doc.
4. I can’t tolerate being patronised – when I’m right and they’re wrong.
4. What difference will one/my Proforma make to a distorted system?
That’s a starter kit.
As you know, I’ve never been harmed myself, but have supported others and endured such encounters. I’ve experienced all the moves – ‘it’s unlikely medication could have that effect’, (akathisia) that’s ‘agitated depression’, medication – induced phonic tics – obviously delusional. A classic – (Psychiatrist) ‘I think a few days in hospital would be good for you’. (Patient) ‘No, that would kill me’. (Psychiatrist) ‘You never know you might enjoy it’. This really happened.
In the end, after watching others endure this behaviour for years – I thought,
**** THAT!
(No prizes for guessing – and apologies to Mary for my uncouth Aussie tone).
Dr. David Healy says
Harriet – Mary
We’ve focussed very much on why people are so nervous to raise medicine related issues with their doctor. There have been RxISK Report and SNOMED initiatives which seem on one level to make perfect sense and seem to offer weapons but they aren’t being used.
Perhaps Mary and Shane’s group offers another option. It began with Mary accompanying Shane to medical meetings. Someone to ensure his message was heard and to stand in the way of the system riding roughshod over him – telling him this is what we the experts things is the case – a message that only leaves him with one option – to conform.
Having two people there makes it easier to stand your ground. To say look we don’t seem to be getting the message over, can we try again. It forces the medical person into being more aware of a need to be ‘decent’ – to concede that the other person’s point of view needs to be taken into account – it forces the medical person to semi-hear the other point of view.
Why not have a trial of someone going along with each of the people in the group to their doctor. Maybe to say nothing, just to be there. It’s not as common now but in all sorts of walks of life we used to have a helping person go with us to things, or be at our side when playing musical instruments or singing through to dealing with the system. The doctor was once supposed to be that person for us but s/he has got or is getting swallowed up by the system.
Having someone there would de-consumerize things. It changes the dynamic back from me being someone going to the supermarket or department store to ‘buy’ something of my choosing. It moves from logic of choice to a logic of care – involving the need to recognize and negotiate our temporary dependence on the doctor not to treat us like a consumer but like a sibling or a friend.
It de-transactionalizes things. We are going to achieve consensus on the right thing to do in this situation rather than saying well I will do something for you in exchange for X amount of rare earth minerals but not otherwise – to use one of the examples of the moment.
If anyone is interested to chase this line of thinking further, one of the greatest books on health care is Annemarie Mol’s The Logic of Care. It’s short, simple and stunning. Not a word of jargon.
David
mary says
I am busy shortening the Rupture article – down to patient evidence only – with a view of getting the group members (many of whom at present have disbelieving members of family) to use it to show that what THEY are experiencing is NOT JUST IN THEIR MINDS!! With such a fantastic opportunity from Harriet, I feel we MUST start at our own feet – hence, your own family/friends. Why shorten it ? -because as a whole piece it is geared towards ALL – professionals and laypersons alike. We need to use this in a variety of ways – to suit different needs, eg – for our area I am adding Prestatyn/North Wales to my heading; for others, that will be left out. I’m also adding my contact detail so that people will know where to get hold of zoom details; further still, there will be occasions to use the whole article – such as CMHT centres. In ALL instances Harriet will be acknowledged as Researcher and the link to the full post will be added. Once I have that in place, it will be over to the individual members to use as they see fit. These “next steps” will be discussed when we next meet, with Harriet, on March 5th. I do see it as my duty to put in the preparatory work and to THEN delegate.
chris says
**** THAT! Yes this is where we are at
https://m.youtube.com/watch?v=r0_T_UOpRp4
‘Just leave me alone’
Dr. David Healy says
Chris
Thanks for this. Its extraordinarily appropriate. If in addition to bringing someone else with us to a consult, we can bring a sense of humor it might help. If we can get a doctor to even hint at smiling, we have probably won – except the next appointment might be with an entirely different doctor. The only way now to get continuity of care is to bring someone with us
David
Harriet Vogt says
Just brilliantly apt, Chris.
As well as very funny.
Harriet Vogt says
Really good suggestion, D.
As you say, visiting the doctor accompanied by a person who knows and cares about you, changes the nature of the interaction.
It doesn’t, in my experience, mean that the doctor will necessarily believe you, but it does mean that they will feel obliged to listen. And you, the patient, just feel safer.
It also fits well with the ethos of Shane and Mary’s group – not having to suffer ALONE.
Annemarie Mol’s ‘The Logic of Care’ has just landed in my kindle. Sitting next to another book I keep meaning to read – Doctor Rageshri Dhairyawan’s ‘Unheard – the medical practice of silencing.’
(Being a bit of a dog with a bone, perhaps we can add a social dimension to the ProForma – a sort of chain letter approach?)
susanne says
Being the ‘ companion’ can be quite nerve racking as some doctors will try to undermine that the person ‘companions’ are there to support him/her by trying to get the companion ‘on their side’ using strategies such as looking at them more or asking for confirmation of something they suggest ‘dont’t you agree? , ‘wouldn’t you think so’?. The companion needs to be absolutely trusted to on their ‘friends’ side so not to be used to sabotage the consultation -but also their own relationship. Maybe this likelihood could be explained to the ‘companion’ so they could be prepared and made wary of the need to maintain their ‘role’ in a consultation. There are many consultations whereby it is perfectly ordinary for friends/relations to accompany someone and to even chip in but to be able to stand back as well as to stand with is vital in consultations such as described on Rxisk where vulnerability and power games are an issue. .
Dr. David Healy says
This is a great point. Tracey Glazebrook often tells about taking a partner to the consultation with her and finding the doctor looks to him for the ‘correct’ answers – trying to get him to agree she is being emotional or hysterical rather than right. Men are fragile vessels so it’s not clear how often you can depend on them to stand up for you.
Many in patient services have advocates but pretty soon after these were introduced over a decade ago. many services found ways to co-opt them into supporting the only rational approach. Ditto with peer support. Advocates and peer supporters now have to agree to support Evidence Based Medicine.
Everyone needs a Tiger Mom.
D
Harriet Vogt says
Critical point.
I’ve found it helpful to treat these medical interactions like a business negotiation.
Pre-decide with the person you aim to support, if able, what we are trying to achieve and construct a tight argument based on patient history, other relevant information about known drug ADEs or whatever. Anticipate counter-arguments – and be prepared to give them short shrift.
This mindset lends a determination and purpose to proceedings – as well as an apparent absence of exploitable ’emotionality’. This is a game of patient safety hardball – not a woolly chat.
Of course, there will be moments when you want to scream – but save this wonderfully therapeutic activity for when well out of earshot.
chris says
The importance of listening in medical care – a Fireside chat with Dr Rageshri Dhairyawan
https://m.youtube.com/watch?v=J6GREwCgItc
Annemarie Mol. Film 1. From Natural Sciences to Philosophy and Anthropology
https://m.youtube.com/watch?v=xauGfgiAzlo
There are quite a few other videos from Annemarie Mol on YouTube if you have duckduckgo you can watch without the adverts.
Lucy Green says
David!
I would like to share some observations with you; I hope you will be patient, reflect on them and take them in the positive spirit with which they are shared.
You have made HUGE strides over the many years of your career, and I think I can speak for all of us in Mary and Shane’s group when are say we are beyond grateful for your commitment and dedication.
BUT I will admit that my first impressions of you have not been favourable. You have slated our group as “women giggling in the kitchen” and as little more than inactive moaners. You have expressed no empathy towards any of us as deeply traumatised souls, here but for the grace of God, because of YOUR profession – which has harmed us beyond description.
However hard you may be fighting to change the psychiatric system David, you remain a PART of it. You are still a psychiatrist, and in the eyes of many of us, you still represent the profession that has nigh-on destroyed our lives. Despite your derogatory and disrespectful comments, I do feel I can trust you – but only because Mary and Shane do, and I trust their judgement, because they have known you for many years. You now seem to expect US, the psychiatric survivors, to do the work. A group of people who are traumatised, terrified, and are fighting endless, largely silent, battles with side effects and withdrawal symptoms.
What is this patronising nonsense about us “hero-worshipping” Mark Horowitz?? Could there be an element of professional jealousy on your part I wonder? As a group, I feel we warmed to Mark and to Peter Scott-Gordon because they both have decent INTERPERSONAL SKILLS. They made a genuine human connection with us. They really understood the hell we have all been through and continue to go through, because they have experienced it for themselves. They really get it. They didn’t mock us, put us down or expect us to come up with the answers. They sat with us where we are at and didn’t judge us.
You seem to be mad at us for our inaction. Please remember that we are barely keeping it together, juggling extreme ill health, family commitments, extreme financial difficulty, and countless other challenges! Speaking for myself, I have never earned a vast amount as a nurse – unlike you doctors, nurses earn relatively little, despite working our fingers to the bone. Thanks to YOUR profession, I have now all but lost my career, and I survive on paltry benefits that I’ve had to fight tooth and nail for, as do most of the group. I am disabled by the drugs that YOUR profession prescribed, yet I also have to bring up two young daughters, one with learning disabilities, and look after my elderly mother-in-law, amongst many other draining family commitments. Since qualifying as a psychiatrist, have you had to manage financial difficulties, or have you benefited massively from a fat NHS salary? Do you wonder where your rent for next month will come from, or how you’ll afford your next meal? Do you agonise about how you’ll manage financially in retirement, or do you have a decent NHS pension? How many psychiatrists, even the more enlightened ones, charge vulnerable people eye-watering hourly rates for private consultations?
When thinking about the male ego, it is oh so easy to blame others for it – your mother, father, or any other group – much harder to actually TAKE RESPONSIBILITY for it – you’re a Big Boy now. Most of us psychiatric survivors have had our souls ripped out and shattered into tiny pieces by the drugs and by our treatment by psychiatry – it has been up to us to piece ourselves back together and the process is acutely painful. How many of you psychiatrists have had to do the same? We’ve had to confront the most toxic elements of our personalities, question everything about our identity. PLEASE, David, acknowledge your ego and vast privilege, and encourage other doctors to do the same!! I wonder if you have really faced the fact that, as a psychiatrist, you yourself will have done MASSIVE harm to countless people, through careless prescription without informed consent? Have you thought about apologising for it? No psychiatrist has ever apologised to any of us.
To move the conversation on with groups like Mary and Shane’s, how about you attend the group again and START with an apology. This is something that none of us have ever heard from any of you. It costs nothing, but it shows EMPATHY, HUMILITY and INSIGHT. It goes a small way towards validating our horrendous experiences. Of course no one expects you to take responsibility for your entire profession. But we need you to hold space for us and show us that you care!
Communicate with us, on a human level! Lose the air of superiority! We are YOUR EQUALS, as fellow human beings. We are very grateful for your knowledge and experience, but first we need HUMAN CONNECTION, warmth, a demonstration of respect. To dismiss us as moaners is yet MORE gaslighting from an overprivileged, quite frankly, ignorant profession who specialises in it.
Mary and Shane have gained our trust and respect because they honour us with theirs and they don’t have a god complex. If at least some psychiatrists could do the same, we might start to get somewhere – with a therapeutic, encouraging relationship. You might just be gobsmacked at what we can achieve, as a COLLABORATION. I’m not saying any of this to slate you – I’m saying it to move things forward.
Best wishes to you
Lucy
Dr. David Healy says
Lucy
It’s good to see a spark of anger from you. What is needed is to direct that anger at the real source of your problems.
I’ve got involved in hosting this Ruptures post because Mary has been angry with the group. Angry at all the moaning and lack of action. She, I and Harriet hoped to get the group to act.
I introduced Harriet to Mary and suggested that her input might help everyone understand what holds all of us back. Harriet’s post came at my instigation.
It has usefully led to a lot things being expressed. A lot of Heat. Any Light? I guess we will only be able to say there has been some light if the group start doing something, start making something happen
David
mary says
David, Lucy and all other readers – can I just explain that my anger was AT THE SITUATION not at individuals within the group. It takes a while to gain a trust each for the other – especially as I have not suffered, but witnessed, the horrors of withdrawal. I now feel that we are getting to be a ‘group’ in the true sense of the word – a group where everyone is of equal importance; a group where those who can, prepare the ground for all to be offered the chance of sharing information outside of our comfort zones. As I explained at last week’s meeting – I now feel a lot happier; I had got to a point where I was asking myself ” what have we done in almost a decade?” and the reply coming back at me was “NOTHING that points towards making a difference”. Actually, I think ‘frustration’ would be a better word to cover how I felt – frustration at the fact that we were not moving forward and at the fact that we were meeting more and more people who were STILL suffering from the same stuff as almost killed Shane 23 years ago.
Now, it’s time to move on – let the frustration/anger subside and put all that energy to better use. Our logo is “Better Times Will return” – let’s ALL work TOGETHER towards it. Working as one, we CAN do it – just as the Wales rugby team ALMOST gave the Irish a good beating yesterday!
Dr. David Healy says
Mary
I know your anger wasn’t at any individual – least of all Lucy. The group is very lucky to have you and Shane and really does need to reflect on the fact that this cannot keep going without an infusion of purpose. The problem for all of us is trying to get to grips with the situational factors that hold us back. It’s beyond the scope of any individual on their own to change things.
Next weeks post about iPADs might shed some light on this and on the increasing difficulties you and the rest of us face when trying to make a difference
David
chris says
Lucy
Looks like they are self imploding here. Psychiatry has no where to go except lie and build ever more prisons. Here it seems as if their arrogance has ruptured out into other external NHS organisations:
https://www.bbc.co.uk/news/articles/cy8nd3vp7jvo
“Throughout 2024, external organisations continued to receive concerns about the trust, mostly anonymously, the trust said in papers for a board meeting, external on Wednesday.
That led to NHS England and the local integrated care board to undertake an investigatory visit in July with a smaller team visiting in September.
The subsequent report found “staff across the organisation consider that the board is not functioning well, and that it is not able to resolve conflicts constructively.
“There has been tolerance of poor behaviours at board and a hesitancy previously to tackle them,” it stated.”
“She said the report highlighted unacceptable behaviours, customs and practices “that, though not universal across the trust, should have no place in our organisation”.
https://www.bbc.co.uk/news/uk-england-birmingham-67660755
“They also have no confidence in the way that the trust has removed its chief medical officer, Mark Weaver.”
“Dr Weaver wrote to the Medical Advisory Committee stating that suggestions he had stepped down were “not true and accurate,” adding “my reputation, nurtured over 40 years and of which I feel I am rightfully proud is being damaged both inside and outside the organisation and I cannot defend myself.”
He had previously applied to be chief executive of the trust, but did not get past the first stage.
He added: “I want to end by mentioning what happened at UHB [University Hospitals Birmgham] and in [Lucy] Letby. In those cases the medical directors sided with management against doctors.
“In Letby doctors were forced to apologise to a nurse who they suspected of murdering babies.”
Can you image being a patient around this lot.. you wouldn’t stand a chance.
How long can this go on ?
Dr. David Healy says
Chris
I think you are pointing to a management culture that is destroying healthcare – turning it into health services. It has very little to do with psychiatry or medicine per se.
Around the year 2010 psychiatry in North West Wales got taken over by an All-North Wales Health Board – Betsi Cadwaladwr University Health Board (Betsi) – based in Wrexham (essentially english). Prior to that we in North West Wales had the lowest bed occupancy in Wales and one of the lowest in the UK. No one had to be shipped out to a bed in England. We had the best staff morale and no vacant posts.
Some years later under new management and a new management approach, there were almost no permanent staff left, there were only locums. Staff morale plummeted. There was a culture of bullying and harassment. The beds were full and lots of people had to be shipped off to england hundreds of miles away at vast expense.
Managers hired management consultants – pals of theirs for lots of money who had been fired from management posts elsewhere. Betsi was put into Special Measures and has spent most of the last decades in Special Measures.
Perhaps if the US celebrities, who know a little about football and I expect nothing about health, who took over Wrexham Football Club, had taken over the health board instead of the football club everyone in N Wales – including Lucy – would be better off.
In a book published in 2012 – I commented in the introduction that in part the book was borne from witnessing the destruction of a good service. Pharmageddon was an effort to get to grips with this.
David
Lucy Green says
David
I still don’t think you are listening. Communication, empathy, human connection – these are everything. Please encourage your colleagues to challenge their ego and develop some humility. I’ve seen it in scores of doctors, as a patient and nurse – this is dangerous, toxic and HAS to change.
Meanwhile, on a personal level, I will do everything in my power to be proactive and to move things forward, and I will encourage other group members to do the same, within the bounds of their considerable limits. But please remember I will be doing this alongside personal battles that you cannot begin to imagine. It’s a thankless slog, every single day. Your profession has caused this and and no mental health professional has EVER offered anything resembling meaningful help. Damn right I’m angry! Psychiatry disgusts me.
L
Dr. David Healy says
L
I’m listening closely and eliciting a response from you that is heading in the right direction but is not there yet.
It’s easy to talk about Mark and Peter being empathetic. Mark wants to make money out of you and others in your position. Peter has tried to get his profession to listen and I have run posts about this. His profession don’t listen to him. They stopped listening to me a long time ago – and have travelled down a path to irrelevance instead.
I’ve been listening to women like Anne Marie and Brianne who have had a lot less healthcare background than you but have done a lot more. Why? They don’t just go around ranting. Hopefully some day I’ll be able to add you to a list of the women I listen to.
D
Lucy Green says
David!
You are infuriatingly arrogant! Hopefully some day I’ll be able to add you to a list of people I can trust and respect.
L
Dr. David Healy says
Lucy
As I just said – your fury might be half way to something useful.
D
David T Healy says
There are parallel conversations happening on The Respiratory Syncytial Virus Challenge post on DH. Harriet has just commented there and suggested sending a note to Mumsnet.
RxISK had a series of Mumsnet posts about SSRIs and pregnancy after a Panorama program on the issue when Mumsnet women were rallying around the drugs blaming anyone who would withhold their supply of SSRIs as ‘misogynists’.
1. The Dark is for Mushrooms, not for Women.
2. Preventing Precaution
3. Mumsnet
4. I’m not Pre-pregnant, I just have a Womb
and much later
5. Lullaby
David
Patrick D Hahn says
Just today there was an article in McClean’s about assisted suicide for depression:
“She stopped using drugs and alcohol and doubled down on treatment (anti-depressant, anti-psychotic and anti-anxiety medication) and therapy (cognitive behavioural, dialectical, art, family, electroconvulsive).”
“Scully has seen more than a dozen psychiatrists and undergone shock therapy 19 times. He takes 30 pills a day, the side effects of which include dizziness, leg spasms, cognitive impairment and slurred speech. ‘I’ve tried everything, and nothing has worked,’ he says.”
In lieu of meaningful help, our society takes distraught, suffering people, and plies them with drugs known to cause worsening depression and suicidality, and when they become despondent and suicidal, we offer them assisted suicide.
https://macleans.ca/longforms/canada-maid-mental-illness/?utm_source=firefox-newtab-en-us
SMH.
Stevie says
Dear David
I know you mention this often but could you please suggest which blogs to read that explain the criticisms of hyperbolic tapering in most detail and suggested alternatives if one abandons this method? The prevailing advice is holding or updosing or micro tapering but at all costs don’t add more meds.
Would like to get a better grasp of alternative views but don’t have a lot of ability ATM. Thank you.
Dr. David Healy says
Stevie
The MiA Webinar post plus video etc in the RxISK post Madness, Normality and Antidepressant Dysregulation followed a few weeks later by Antidotes for Akathisia and Dysregulation.
Some people can stop without tapering. These may be largely the people who do not have other damage as evidenced by PSSD or VSS or other problems. Tapering even often years does nothing to alleviate or remedy this damage. In between then when there are clear difficulties it makes sense to taper at an individual pace – not a hyperbolic pace. Peter Groot’s tapering strips can help with this.
What is clearly happening in lots of cases is that SRI and related drugs do lots of other things and hyperbolic ideas don’t take any of this into account. It seems increasingly clear that antidotes can help some of these other things – but antidotes are not going to be antipsychotics, other antidepressants or whatever. The Antidote post might offer some insights.
The XXX mysteries of tapering post offers additional points pertinent to women. I had hoped to be able to add to this and hopefully will soon.
D
Paul says
Sorry if this has already been answered but does the Rxisk Map (of good practioners) exist and if so, where can I find it please?
Dr. David Healy says
Good question and I’m going to repeat your question and this answer in response to the next RxISK post later this week.
We had a RxISK Map from very early on but it didn’t get used. We pushed this idea again in 2017 –
see https://rxisk.org/rxisk-map-relationship-based-medicine/
We even had a paid plug-in which showed a world map and let you Zoom in to your area but it didn’t get used. We have now disabled it as it cost too much money.
We have a list of doctors open to getting PSSD referrals – a PSSD map – see RxISK Toolbar. But this just takes your suggestions of doctor’s names where the RxISK Map asked for proof – getting a doctor to fill their bit of your RxISK report form.
Either you and everyone else is too scared to do this or doctors are just not willing to do it – perhaps too scared – but we didn’t get any Doctors ending up on the Map when this was the eye of the needle through which they had to pass.
I will be interested in comments from anyone reading this – but not cheap comments – they need to engage seriously. Especially interested after the next post where these same issues come to a head.
D
Lucy Green says
David!
I would like to apologise, for blowing my top at you the other day. I reacted to your comments by vomiting 16 years of pent-up anger and frustration all over you, at the torture I’ve been put through by psychiatry – of course it’s nothing to do with you, you were just there at the right/wrong time!
I wanted to let you know some of the things I have done since waking up to the adverse effects of antidepressants (and psychiatric drugs in general). I have written countless letters to psychiatry and to GPs, telling them about my experiences of psychiatric harm and trying to inform them of the dangers of antidepressants (including sending Katinka’s book to several psychiatrists). I had an article published in the Guardian about my experiences of postnatal psychosis and I took part in a short film to give hope to people suffering with mental ill-health (sadly, it was before I realised the drugs were the cause, but my intentions were honourable). I’ve spoken to groups of psychiatrists and other mental health professionals about the hell of my experiences. I have tried to warn friends and family about the dangers of antidepressants through my writing, social media posts and discussion. As a practice nurse, I’ve told numerous patients and colleagues about the potential adverse effects of antidepressants and the dangers of withdrawal, going against mainstream thinking. I’ve written to my psychiatric teams many times to challenge inappropriate diagnoses and polypharmacy (and have mostly been ignored). As an inpatient and in depressive psychosis, I tried to reach out to as many fellow inmates as possible, knowing that most of their suffering was likely caused by the drugs. I’ve written to countless people online to inform them of the dangers of venlafaxine and the need to withdraw very slowly.
I’m not telling you any of this to Big Myself Up; I’m just trying to help you see that there is MASSES of positive work going on behind the scenes – I’m just one of tens of thousands of psychiatric survivors who are helping to get the message out there. We may not be an organised group (YET!), but many of us are busting a gut to challenge the status quo, even though it is massively triggering for many of us to do so – we are pushing ourselves right out of our comfort zones and we risk making ourselves (more) ill in the process. After decades of working like a trojan, I wouldn’t be at all surprised if you feel a little worn down/jaded by it all. I know you don’t think I am worth listening to (yet), but I’ve taken a punt and thought it was worth telling you this. I really hope my previous comments didn’t stress you out too much.
Very best wishes and thank you for all you do for us.
Lucy
Dr. David Healy says
Lucy
You don’t even need to begin to think about apologizing. We are all in a terrible situation.
A particular problem is that given so many people have such significant even potentially lethal problems, why are the medical and political systems ignoring us when we ask them nicely/politely to pay heed to what is happening. And why can we seemingly do nothing or so little when we demand they look our way and pay heed?
You’ve outlined very vividly just how little the system listens. We desperately need to find a way to get the system to pay more heed to voices like yours.
It’s great for me to have another woman whose example I can point to as illustrating what we are up against and demonstrating the kinds of things that need doing
David
chris says
“A particular problem is that given so many people have such significant even potentially lethal problems, why are the medical and political systems ignoring us when we ask them nicely/politely to pay heed to what is happening. And why can we seemingly do nothing or so little when we demand they look our way and pay heed?”
Just watching PMQ’s and a question on preventing suicide
… reply more SPECIALLY’ trained mental health workers are to be employed. How many times have we heard that. All the answers are on here and nowhere to be found on NHS England nor NICE. Is anyone going to employ me/us? Even if they did I don’t want to work for the NHS after what I suffered.
Lucy I’ve been at this for over 14 years and only two people have ever replied to my emails about recognising akathisia as a major cause of immense suffering, suicide and violence. It’s very difficult to realise it is only people who have suffered SADR’s and those who died, their families, partners and friends who want to know about all this.
Think they are well aware of a massive tidal wave of litigation if any of this is admitted. Think they will just keep on with the above. It’s just too horrific to face upto rather like slavery. But my emails will keep going.
Dr. David Healy says
Chris
I’m not trying to trump either Lucy or you but I’ve been at this over 3 decades publishing peer reviewed articles and being an expert witness. A quarter of a century ago I lost a job because of it. I’ve been referred to the GMC and other regulatory bodies several times
We have to stand together or we will hang separately. The task is to find a way to make standing together effective.
The next 2 RxISK posts will add to the debate – will point to what we are up against
David
Lucy Green says
I agree Chris. I’m so sorry for your suffering. I’ve given up my career as a practice nurse, because of ill health from venlafaxine withdrawal etc but also because I can’t live with the constant blanket, thoughtless prescribing in GP land. Precious few in mental health services seem prepared to listen to us, but like you I will keep on writing/emailing because even small actions will have some impact eventually, and we are not alone. People like David are having a massive rallying effect. He and Peter Breggin saved my life, by revealing the truth about the drugs in films put up on YouTube. Let’s hope poor old David never retires!
Lucy Green says
I drafted an email to PALS this afternoon about challenging the diagnosis of schizoaffective disorder I was randomly given by a psychiatrist last year – after one brief conversation with me and without any discussion with me about the appropriateness of the diagnosis. Two things occurred to me. If we need certain outcomes like this from psychiatry, are we best off going through PALS to have them registered as complaints, so that more people in mental health services are made aware of them, or even to address our concerns to the chief exec? And… am I pussyfooting around being too polite when I request things from psychiatry or from my GP? – as the expert in my own health, should I be demanding things much more assertively, in the way doctors seem to do? Perhaps I’ll try both these approaches, and see if they make any difference.
Harriet Vogt says
Challenging a diagnosis – even one dished out hastily and sloppily as mashed potato in a canteen, like yours clearly was, Lucy – is your right, as a patient, your human right as a person – but a bit of a performance.
I just remembered this useful MiA piece by Jo McFarlane from a couple of years ago- literally a step by step guide to https://www.madintheuk.com/2022/09/challenge-psychiatric-diagnosis/.
‘…as my psychiatrist somewhat sheepishly admitted when I pressed him on the matter, ‘Psychiatrists just go with their hunch about a patient’. We can interpret that as ‘blatant prejudice and bigotry’. They are quite literally, a law unto themselves. So, let’s start holding psychiatry to account and take some power back over how we choose to self-define.’
It’s worth taking the time to challenge the system in a way it cannot ignore. But a rough blast of rage on a page first, during and after, is highly recommended and very therapeutic.
Perhaps best to think about recipients after you’ve written it. PALS alone is too lowly.
susanne says
I used to work for the Community Health Council in England before it was disbanded and dis-empowered by setting up the farce of so called independent advocacy services and tokenistic peer groups. Some of us set up advocacy groups independently but were too undermined by them as were those who used them to take this further .
There is though only in Wales another similar group as the CHC ‘s which has done some decent speaking out called Lais in Wales. Sometimes it depends on the quality of those running the organisation so I am not up to date on that.
Llais Wales | Llais
Llais Wales
https://www.llaiswales.org
We’re here to make sure your views and experiences are used by decision-makers to plan and deliver better health and social care services.
About Us · Contact us · Make a complaint · Come and work for us
chris says
Might find this an interesting read. Any nurse’ in the UK caught doing that would be struck off, but if they are involved in drug harms or physical restraint harms it’s part of the job nothing to see here:
https://www.artnews.com/art-in-america/aia-reviews/anna-odell-psych-ward-kunstmuseum-trondheim-1234733578/
Laura says
Some interesting views. Whilst I recognise withdrawal can be extremely challenging. I’ve been on these drugs(SSRIs) for years now because I can’t get off them without severe withdrawals. I went on them for mild stress/anxiety due to job pressure. I now sink into a depressive and suicidal state every time I’ve tried to get off them. This is just the psychological withdrawal. Physical issues include my digestive system, bodily twitches and brain zaps to name a few.
The whole withdrawal subject , community and forums are nuanced. I’m not entirely convinced on the idea of waves and windows in its rigid sense and the expectation they should perhaps disappear once withdrawal eases. Life is full of ups and downs(windows and waves) and I think if someone is under the impression that they must go to be classed as ‘healed’ risks creating a false illusion and expectations.
Life will always have waves(hard times)and this could be misconstrued as withdrawal which is lasting years and years. When this may just be life.. Whilst I am no Dr and I am not questioning that withdrawal can come with these ups and downs we can’t be under a false illusion life will be forever good.
For example someone might have a tough period in their life which triggers extreme emotions, emotions they may not have had full range to whilst on medication. This may come as a shock and the person may think they have hit another wave and sink into hopelessness. As I say it’s nuanced.
Forums can be helpful for sure especially around validation and support but there are many voices out there and not everything you read will be true. It can get very muddy trying to distinguish what is withdrawal and what is just life. People can get mixed messages from online forums. I think you have to keep an open mind when in forums and stay mindful they are a place often full of pretty frightened people with different views, motives and experiences.
ANON says
Once the rupture has happened, it’s not a simple matter of stitching things back together and pretending nothing has ever happened. Once the damage is done, that it! Sadly, you are rovinato (ruined)!
We have a system that is totally up the creek!
I ask myself this question, over and over again: Why for heaven’s sake, can’t these experts who have an in-depth knowledge of antidepressant withdrawal and the risks of polypharmacy, be in every place at one given time?
The problemo we have is that there are too many people in denial and if we still educate and try to open up the eyes, they are still going to rub it in your face and rubbish everything you know about the subject matter.
Mamma Mia, we have a long way to go, and it sucks!
Experience counts more than a piece of paper on the wall, but some people don’t give a rat’s ass!
What do we have to do to open up people’s eyes?
Mamma mia, some people are still asleep because IGNORANCE is bliss!
It should not be a frightening experience, if some people just took the bloody time to listen instead of ridicule and mock.
If we humans don’t learn now, when are we ever going to bloody learn?
Thank you, David, for giving us this forum to vent because I honestly don’t know how to get through to people ~ it’s like they just don’t bloody care!
They twist the narrative, always having a smart-ass answer to throw back at you.
The problemo is, if you do not follow the rest of the bloody heard, you are considered pazzo (crazy)!
Who cares!
As far as I am concerned, some don’t care if the rapture keeps getting bigger.
As long as it does not impact them however, when it does ~ modus operandi; Who cares!
Carla says
The only way we can repair raptures in medical care, is if:
1. The culture in clinical care changes. Doctors need to listen to their patients and health care needs. When
they are trying to explain that the medicine(s) or procedures are causing harm, patients need to be heard
not dismissed.
e.g.: If someone is in so much pain, please don’t tell them it is depression, anxiety or psychosomatic and
send them on a wild goose chase with tests and procedures that are invasive, which may cause more
harm than good.
2. The Law regarding policies with how patients are compensated has to change. If the medical procedure or
medicine (s) have maimed or induced death, those who have suffered or loved ones who have endured
the suffering with them, need to be included as part of the compensation process.
3. The cover-up’s, lies and deceit need to be exposed and those who have been injured need to be heard not
given the run around.
Many decades ago, people similar to me, put medical professionals on a pedestal and we did what we were told to do because we thought they knew everything. This is not the case. We listened to our health practitioners and assumed that everything they said and did was right.
Now, you have people judging us.
We suffered and endured so much. There are no words to express how we fee, today.
We were left behind.
We were abandoned by the health professionals, the Government, families and some friends.
There was no compensation for injuries we were left with from procedures or medicine(s) that maimed or induced unnecessary deaths. Now, you can understand why, we don’t trust!
Many decades later, we have made little progress and are still witnessing the same cultures, laws and destruction of what some procedures and medicine(s) induce.
Many are still not being heard today and until we see dramatic changes in our health care system, the rapture in clinical care will sadly continue.